BCBA Scope of Practice for Grief Work: What You Can and Cannot Do
Plain language guide to the BCBA scope line for grief support. What you can do, what you refer out, and how to stay ethical, from a BCBA-led CEU.
Key takeaway
As a BCBA, you can track and reduce grief-related behaviors, but you cannot treat the feelings underneath them or diagnose prolonged grief disorder. That is the line, and this page walks you through it.
Increasing Competence and Confidence in Helping People with Disabilities through Grief
On this page · 12 sections▾
BCBA Scope of Practice for Grief Work: What You Can and Cannot Do
As a BCBA, you can track and reduce grief-related behaviors, but you cannot treat the feelings underneath them or diagnose prolonged grief disorder. That is the line, and this page walks you through it.
If a client is acting out after a parent died, that is your lane. If a client is stuck in painful feelings six months later and cannot move forward, that is a referral to a Licensed Professional Counselor (LPC) or another mental health practitioner. Same family, two different jobs.
What this page covers#
- Why grief work feels like a gray area for BCBAs
- What BCBAs cannot do: process emotions, diagnose prolonged grief disorder
- What BCBAs can do: track grief responses as observable behavior
- Topography and frequency changes after a death loss
- The behavior analytic definition of a grief response
- When to refer to an LPC or mental health practitioner
- How to document that you stayed inside scope
- Red flags that you have stepped over the line
Why grief work feels like a gray area for BCBAs#
Most BCBAs were trained on skill acquisition, problem behavior, and parent training. Grief did not show up in the textbook. So when a caregiver dies and the client starts hitting, eloping, or shutting down, the team looks at you, and you freeze. Is this behavior or is this something bigger?
It is both. And the field is just starting to catch up. The early research came out of the UK, and there are still only a handful of behavior analytic papers on the topic. That gap is why teams default to medication or restriction when a grieving client acts out, instead of treating the response as human.
Until the 1970s, the assumption was that people with disabilities did not grieve at all. The reasoning was that they could not understand death, so the behavior changes after a parent died were chalked up to the disability itself. We know better now, but the old habit still lingers in care teams. That is part of why scope confusion shows up so fast. If staff do not see the death as the cause, they treat the response as a behavior problem and reach for a behavior plan. You are the person who can name what is really happening.
What BCBAs cannot do: process emotions, diagnose prolonged grief disorder#
There are two hard walls. You cannot sit with a client and help them talk through how sad they feel about their dad dying. That is therapy, and it belongs to LPCs, social workers, and other licensed mental health practitioners. You also cannot diagnose prolonged grief disorder or complicated grief. Those are clinical diagnoses with specific criteria, and they sit outside what a BCBA is credentialed to assess.
We're not therapists. And so it's not our goal to help someone process their feelings of grief. From the talk — Patricia Lund
We also can't diagnose. There's some very specific disorders related to grief, prolonged grief disorder, complicated grief. From the talk — Patricia Lund
If a client needs either of those things, your job is to know the wall is there and to bring in the right professional. That is not a failure. That is the ethics code working.
What BCBAs can do: track grief responses as observable behavior#
Here is where you actually get to help. Grief shows up as behavior, and behavior is your home turf. You can run frequency counts, ABC data, and topography measurements just like you would for any other behavior of concern. You can build interventions that protect the client from secondary harm, like losing phone privileges because staff misread crying as noncompliance.
What we can do is we can look at behaviors and we can provide input about how frequently behaviors are happening. Has the topography of a behavior changed since the death loss happened? From the talk — Patricia Lund
You can also advocate. When group home staff or parents say "they are just having behaviors," you can be the person who connects those behaviors to the death loss and asks the team to slow down before adding restrictions.
There is real work to do on the environment, too. Secondary losses pile up fast after a primary loss. The client may lose transportation, contact with the caregiver's friends, financial control, the daily morning text message, or the routine of weekly visits. Each of those losses is its own behavior trigger, and each one is something a BCBA can mitigate. Arrange new transportation. Map out who can take over the visits. Build a visual support network the client can see and the staff can follow. That work is squarely inside scope, and it often does more for the client than any direct behavior plan would.
Topography and frequency changes after a death loss#
This is the data question that tells you a behavior is a grief response. Ask two things. First, has the topography changed? Crying that used to be quiet is now loud. Aggression that used to be open-hand is now closed-fist. Eating that used to be steady is now refusing meals. Second, has the frequency changed? Are you seeing more elopement, more isolation, more property destruction than baseline?
Watch for less obvious shifts too. A teen who suddenly says "I don't care" about everything. A client who avoids any older man because grandpa was an older man. A client who keeps asking where mom is six weeks after you already told them. A grief burst that hits three or six months after the death, when the brain finally catches up to the permanence.
These are real, and they are measurable. Log them. That data is the evidence that lets you advocate and stay inside your scope at the same time.
The behavior analytic definition of a grief response#
Karola Dillenburger and Mickey Keenan describe a grief response as a mix of private and public behaviors that show up after a death loss. Public behaviors are the ones you can see and count: crying, yelling, aggression, withdrawal. Private behaviors are the internal ones the client may or may not be able to describe: thoughts, body sensations, the urge to hide.
You only get to work on the public side. But the private side is real, and ignoring it is how teams end up punishing a feeling. So your job is to count what you can see, name what you cannot, and write a plan that respects both.
When to refer to an LPC or mental health practitioner#
Refer out the moment the client needs help with the feelings, not the behaviors. Some clear triggers:
- The client wants to talk about what happened and how they feel about it
- Grief responses are still intense six months later and not fading
- You suspect prolonged grief disorder or complicated grief
- The client has a trauma history that is showing up alongside the grief
- The family wants counseling, not behavior support, and is asking you for it
When you refer, do not just hand off the name. Offer to consult with the LPC so they understand how the client communicates and what reinforces them. Many counselors have not adapted their methods for clients with intellectual or developmental disabilities, and your input is what makes the referral actually work.
If the client is nonspeaking or uses AAC, send a brief on their communication system, their typical pace, and the sensory factors that help or hurt sessions. If the client has a history of trauma, share what you know with consent so the counselor is not starting from zero. The goal is a handoff that holds, not a name on a piece of paper that the family never follows up on.
How to document that you stayed inside scope#
Documentation is how you protect the client and yourself. Three habits make this clean.
First, write your goals in behavioral terms. "Reduce frequency of property destruction following caregiver death from X per day to Y per day," not "help client cope with grief." The language matters.
Second, log every consult or referral. Note who you talked to, what you shared, and what they recommended. If you brought in an LPC, name them in the file.
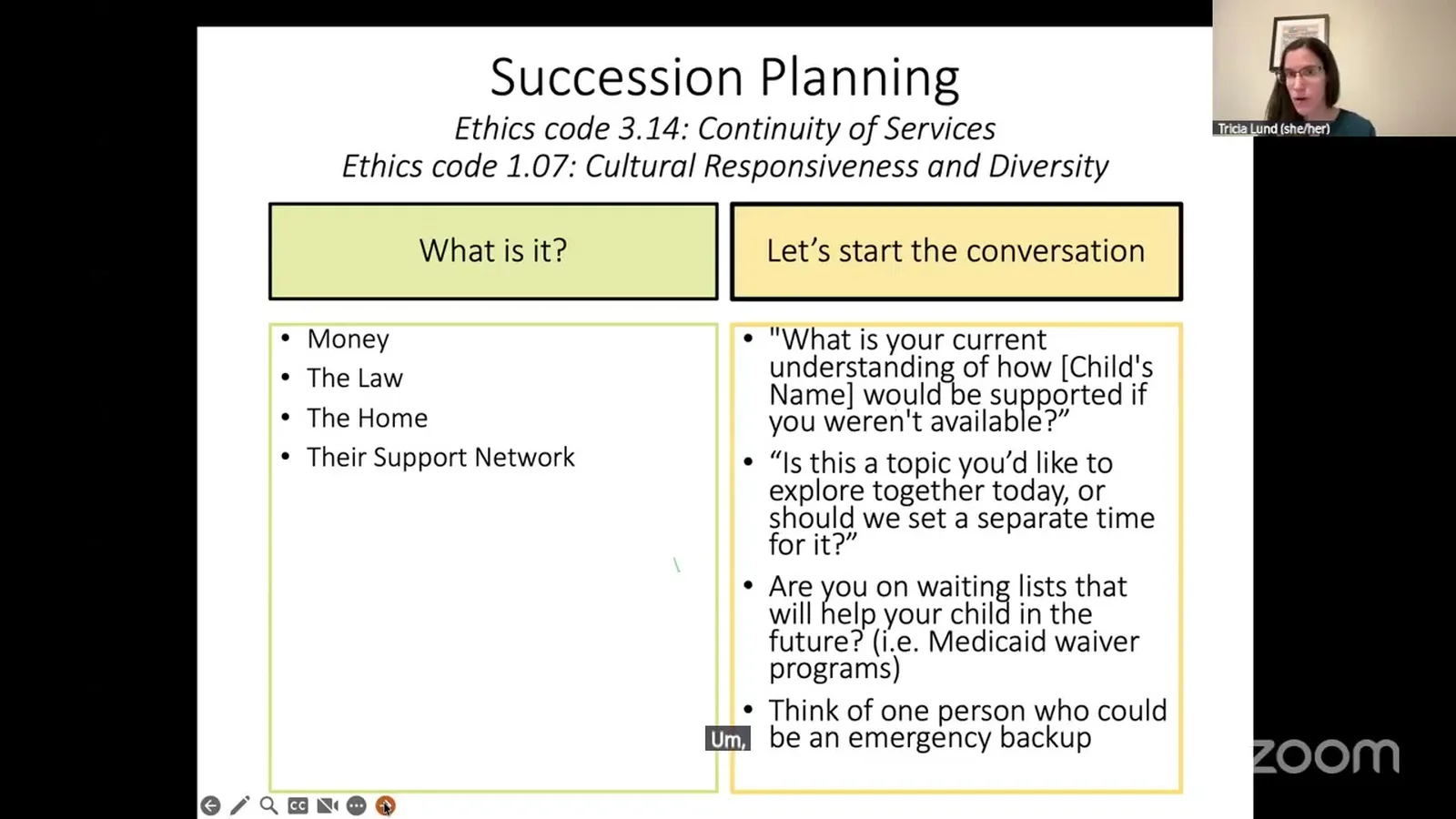
Third, keep your interventions tied to environmental variables: support network maps, transportation plans, staff training on grief responses, succession planning conversations with caregivers. Those are all inside your scope. Processing feelings is not.
Red flags that you have stepped over the line#
You have likely drifted out of scope if you find yourself doing any of these:
- Asking the client how they feel about the death and trying to help them work through it
- Telling the family the client has prolonged grief disorder or any other clinical condition
- Running a "grief therapy" session instead of a behavior session
- Writing a goal that targets emotional processing rather than observable behavior
- Skipping the referral because you feel like you can handle it yourself
Notice them, stop, and bring in the right professional. The work you can do inside scope is meaningful on its own. You do not need to expand the lane to be useful.
BCBAs can really improve their competence and really help the adults that they work with. From the talk — Patricia Lund
FAQ#
Is grief work in the BCBA scope of practice?
Yes, with limits. You can assess and intervene on observable grief responses, train staff and caregivers, and coordinate with mental health practitioners. You cannot do talk therapy or diagnose grief disorders.
Can a BCBA diagnose prolonged grief disorder?
No. Prolonged grief disorder is a clinical diagnosis that requires a licensed mental health practitioner. A BCBA can flag concerns and refer, but cannot make the call.
Can a BCBA help a client process feelings of grief?
No. Processing feelings is the work of an LPC, social worker, or other licensed therapist. A BCBA helps by reducing harm from grief-related behaviors and connecting the client to someone who can do the feelings work.
What grief activities are clearly inside the BCBA scope?
Frequency and topography data, support network mapping, succession planning conversations with caregivers, staff training on grief responses, environmental adjustments to reduce secondary losses, and consultation with the client's broader care team.
When should a BCBA refer out to an LPC?
When the client needs help with feelings rather than behaviors, when responses are still intense six months out, when prolonged grief or complicated grief is suspected, or when trauma is layered onto the loss.
Related guides#
Watch the full CEU#
Patricia Lund walks through the behavior analytic view of grief, the ethics code anchors, and the interventions that actually help adults with disabilities after a caregiver dies. One free ethics CEU.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Increasing Competence and Confidence in Helping People with Disabilities through Grief with Patricia Lund and earn a free BCBA CEU. Detailed certificate, delivered the moment you finish.