BCBA Confidence in Grief Work: Beating the Imposter Voice When You Take a Case
Most BCBAs feel underqualified to support a grieving client. Here is how to build real confidence, not fake it, from a BCBA-led CEU.
Key takeaway
A live viewer named Matt typed it out in plain language during the CEU: his competency was not close to where it needed to be, and it was hard to feel confident.
Increasing Competence and Confidence in Helping People with Disabilities through Grief
On this page · 10 sections▾
A live viewer named Matt typed it out in plain language during the CEU: his competency was not close to where it needed to be, and it was hard to feel confident. If you have ever stared at an intake form for a grief case and felt the same way, you are in good company. Matt was not the only one in that chat who said it. He was just the one who said it first.
Most BCBAs who take a grief case carry a quiet, ugly thought into the first session. The thought is that you are about to do harm because you are not ready. That feeling has a name, and it shows up in every helping profession. The fix is not to wait until the feeling goes away. The feeling does not go away by waiting. The fix is to build small, real reps inside your scope until the imposter voice runs out of evidence.
This guide is for the BCBA who already cares, already studies, and still feels like a fraud the day a family asks for help with grief.
Why almost every BCBA feels like a fraud on their first grief case#
Grief work feels different from a feeding protocol or a token system because there is no clean prompt-and-reinforce cycle. A client is sad. A parent is gone. A staff member is asking why the behavior plan is not working. You do not have a graph that says you are doing it right. So your brain reaches for the worst story it can find, and the worst story is that you have no business being in the room.
Patricia Lund named this directly during her CEU. She said the brain spins up shame and tells you to know all the things now, and then you freeze. That spin is the imposter voice. It is not data. It is a setting event for shutdown.
If you feel yourself doing that, maybe you don't, maybe I'm the only one, but if you see yourself doing that, just take care of yourself. Notice that the thoughts are coming from a place of love.
The first move is to label the feeling, not the person. You are not a fraud. You are a behavior analyst hitting a new area of practice that your master's program almost certainly did not cover.
Confidence is built on small reps, not big credentials#
Confidence is a learned behavior. Like every learned behavior, it grows from contact with reinforcement. Reinforcement in a grief case looks like a parent saying the staff finally understood what was happening, or a client tolerating a transition that used to spike behavior. Those are small wins. Stack enough of them and the imposter voice loses volume.
This is why waiting on another credential rarely fixes the feeling. A new certificate is a one-time bump. Reps are a stream. You want the stream.
Start with what you already do well: take data, run a functional view, write clean intervention notes. Apply those exact skills to a grief case. You will be uncomfortable. You will also notice that your existing skill set carries more weight than your imposter voice gave it credit for.
The five competence floors: knowing you can stay inside scope#
Here is a floor-by-floor read on what a BCBA can do on a grief case without crossing into therapist work.
- You can define grief in behavior analytic terms. Grief is a set of respondent and operant changes after the loss of a major reinforcer. That is your language.
- You can identify setting events that change how a client grieves. Trauma history, where the death happened, relational dependence, culture, secondary losses. All inside your training.
- You can describe why a caregiver death drives challenging behavior. Lost reinforcers, ripped support network, new staff who do not know the client, contrived punishments that punish a grief response.
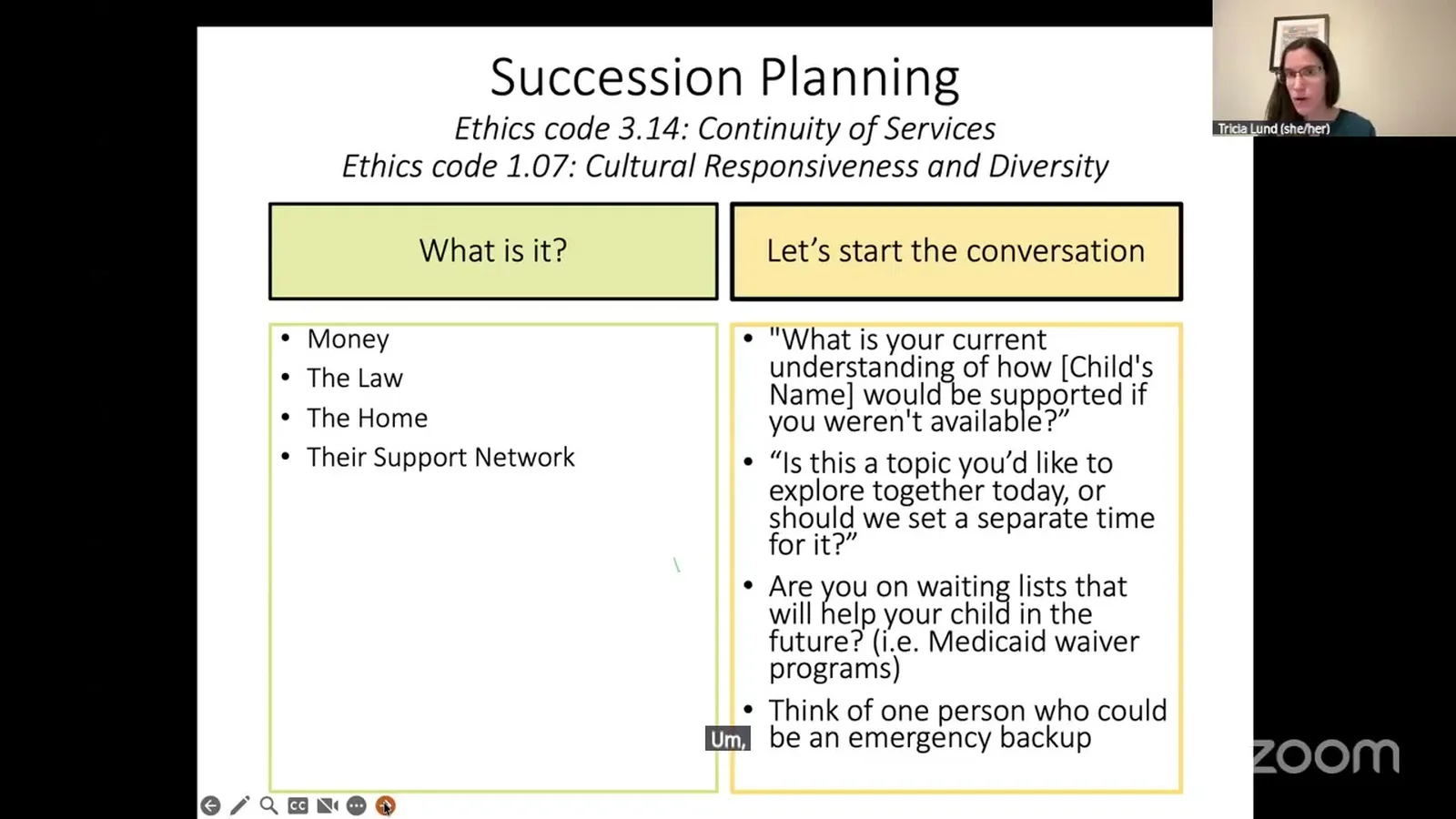
- You can choose interventions that fit your scope. Succession planning trainings, visual support networks, advocacy with group home staff, secondary-loss mitigation.
- You can refer out for the work that is not yours. Diagnosis of prolonged grief disorder. Processing emotions in a therapy frame. That belongs to an LPC, mental health practitioner, or social worker.
If you can speak to each floor in a sentence, you have the floor under your feet. That is competence. The credential police are not coming.
Reframing guilt and shame into a growth signal#
The CEU said this in one of the cleanest lines of the hour.
When we know better, we do better. We're going to be learning about some different ways to view things. Don't let the guilt and shame impact you. If that's what you tend to feel, use it as a way to grow.
Guilt and shame are private events. They are also data. They tell you which corner of your practice you care about. If you felt nothing on a grief case, that would be the real problem.
Turn the guilt into a one-line action: read one paper this week, sit in on one peer consult, watch one CEU recording. That is the rep. The shame does not survive contact with a finished rep.
How to take a grief case with a senior consultant on speed dial#
You do not have to do this alone. Almost no one does it alone well.
Before you say yes to a grief case, line up three things.
- A peer BCBA who has at least one grief case under their belt. Their job is to read your notes and tell you when you are drifting toward therapist work.
- An LPC, social worker, or mental health practitioner in your client's area. Their job is to take the emotional processing side of the case. You hand off, you do not absorb.
- A short reading shelf. Maureen Oswin's work on grief and disability. The Dillenberger and Keenan papers on a behavior analytic view of grief. One book on succession planning.
With those three in place, you are not the lone clinician on a hard case. You are a coordinated team member, which is exactly what the ethics code asks for.
Tracking your own competence growth case by case#
You take data on clients. Take data on yourself.
Pick three to five things you want to get better at over the next two grief cases. Examples: I will name secondary losses out loud during intake. I will avoid euphemisms and use the word died. I will write a one-page succession planning starter for the family. I will schedule one consult call per case. I will train staff on what a grief response looks like.
Score yourself after each case. One to five, no commentary. Watch the line move. The line moving is the data that finally outvotes the imposter voice.
What to say to a parent who asks if you have done this before#
This is the question that freezes most BCBAs. Here is a sentence you can borrow.
"This is a growing area in our field, and I am committed to it. I have done X cases like this, I work with a consultant on cases like yours, and I refer the parts that are outside my scope to a licensed therapist. Here is what I can do, here is what I cannot, and here is who handles the rest."
That answer is honest. It is also evidence that you are a safe professional to hire. Parents are not asking for a perfect resume. They are asking whether you will tell them the truth and whether you have a plan.
This is a new area in the field of ABA.
That line came straight from the CEU. Naming it is part of the answer.
When low confidence is actually a useful warning#
Sometimes the imposter voice is wrong. Sometimes it is right.
If the case involves active suicidality, a diagnosable mental health condition that needs treatment, or grief that has rolled past a year with no movement, your discomfort is signal. That is not a case to white-knuckle. That is a case to co-treat or refer. Low confidence in that moment is a feature, not a bug.
The skill is telling the two voices apart. The imposter voice says you should not be in any room. The useful warning says this specific room needs another professional too. The first voice you push through. The second you act on.
FAQ#
Is it normal to feel like a fraud on a grief case? Yes. Almost every BCBA does on their first one and most do on their fifth. The feeling means the work matters to you. Use it as a prompt to prep, consult, and read, not as a prompt to pull out.
How long does it take to feel confident with grief support? There is no fixed timeline. Most BCBAs report a meaningful shift after three to five cases with consultation and reading on the side. Confidence tracks with reps, not with weeks on a calendar.
Should I tell the family this is my first grief case? Be honest without dumping. You can say that grief work is a growing area in the field, that you have prepared for cases like theirs, that you work with a consultant, and that you refer out the pieces that are not in your scope. That is enough.
What is the minimum I should know before saying yes to a grief case? A behavior analytic view of grief, the difference between primary and secondary losses, the parts of the ethics code that govern scope, who you would refer to for the therapy piece, and a starter framework for succession planning. If you have those, you have a floor to stand on.
How do I keep imposter syndrome from making me overpromise? Write the scope line in your intake notes before the first session. Decide in advance what you will do, what you will not, and who you will refer to. When the parent asks for more, you read the line instead of inventing on the spot.
Take the CEU and stack your first rep#
The fastest way to move from feeling like a fraud to feeling like a coordinated team member is to put real instruction behind your next case. Patricia Lund's free CEU walks through the behavior analytic view of grief, the ethics floors you can stand on, and the secondary loss strategies that actually move the needle.
Watch the free CEU on confidence and competence in grief work and use it as your first prep rep before the next case lands on your desk.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Increasing Competence and Confidence in Helping People with Disabilities through Grief with Patricia Lund and earn a free BCBA CEU. Detailed certificate, delivered the moment you finish.