Anxiety vs Avoidance in ABA: Why Treating Them the Same Backfires
Anxiety and escape-maintained avoidance look the same on a data sheet but need different plans. Here is how a BCBA tells them apart, from a BCBA-led CEU.
Key takeaway
Two kids, same data sheet, two different drivers, and the plan you wrote on Monday for one of them will quietly fall apart on the other by Thursday. That is the whole problem with anxiety vs avoidance in ABA.
Hey, Chillax Man! Understanding the Logic of Anxiety
On this page · 9 sections▾
Two kids, same data sheet, two different drivers, and the plan you wrote on Monday for one of them will quietly fall apart on the other by Thursday. That is the whole problem with anxiety vs avoidance in ABA. A board certified behavior analyst (BCBA) runs a functional assessment, sees a clean escape pattern around demands, writes a tight skill based treatment (SBT) plan, and ships it. In Matt's clinic with one kid, the SBT plan worked the way the textbook promised. In a school case with a kid who looked almost identical on paper, the same plan collapsed inside four days. The behavior data looked the same. The driver underneath was not.
This page is the diagnostic fork in the road. It is for the working BCBA who has to walk into a meeting tomorrow morning and say, "I do not think this is plain escape, I think there is anxiety underneath, and here is how I know." It is not the page on the mechanism of anxiety, and it is not the page on how to build the step ladder of exposure. Those live next door. This is the page that helps you call it correctly before any of that work begins.
The short version: same data sheet, different driver#
When the data sheet says "behavior occurs when demand is presented, behavior terminates when demand is removed," most BCBAs read escape. That read is often right. Sometimes it is wrong in a specific and costly way. The behavior is still terminating the demand, but the reason the kid is desperate to terminate it is not the demand itself. It is a wave of internal arousal that the demand kicked off. The escape works because it turns the wave off, not because the worksheet was hard.
Dr. Sigaud frames this carefully so we do not slip into the old habit of treating anxiety as a function.
So anxiety isn't really the same as a function of behavior, nor is it just sort of this catch all box of mystery that motivates certain behavior. It's a word that describes a set of circumstances and motivations that are derived from our evolutionary past and the way our brains and our bodies work now. From the talk — Dr. Clelia Sigaud
Read that again. Anxiety is not a function on your FA form. It is also not a magic box you point at when nothing else fits. It is a name for a real physiological state with a real shape, and that state interacts with negative reinforcement in a way that looks identical to plain escape until you know what to look for.
What plain escape-maintained behavior actually looks like#
Plain escape is loud, fast, and tied to the demand in front of the kid. The worksheet hits the desk, the kid throws it, the worksheet leaves, the kid calms down inside a minute. Heart rate comes back. Eye contact returns. The kid will accept a different demand right away if it is easy. Pull the same worksheet back out an hour later and you get the same fight, the same speed, the same recovery. The behavior is doing one job for the kid, and it is doing it well. You can shape your way out of this with a standard SBT plan. You teach functional communication, you build tolerance, you fade demands back in, and the data bends.
Matt had a kid like this. The plan ran the way it was supposed to run. The kid earned the steps. The team got confident. Then a second kid came in with a profile that, on the intake form, looked almost the same.
What anxiety-driven avoidance looks like in the same kid#
The second case looked like escape and was not. The trigger was not really the worksheet. It was the wave of internal arousal the worksheet set off, and that wave did not turn off in a minute. It did not turn off in ten. Once it started, the kid was not in the room with you anymore in any useful sense. Matt's read on the moment, after the fact, was the bedside test for the whole article.
When he was escalated and when he was really concerned, it was like he shut off all of his mental processes and could only think about one thing. And that was to get out. Hindsight being 20-20, that really seems like a fight or flight response, like a physiological shutting down of the body in order to get out of a dangerous situation. From the talk — Dr. Clelia Sigaud
That is not Tuesday afternoon escape behavior. That is a body in the red. Heart rate up, attention narrowed, no access to the higher order skills you were planning to teach. You can put the worksheet away, and the kid is still in the wave for another ten or twenty minutes. You can offer a preferred item, and it does not register. The escape worked, but only sort of. The demand is gone, the wave is not.
The tell is in the recovery curve. Plain escape recovers fast. Anxiety driven avoidance recovers slow, and the next exposure to anything that even resembles the original demand kicks the wave off again, sometimes harder. That is the loop that breaks a standard SBT plan.
The cookie test: why arbitrary reinforcers fail with anxiety#
Here is the cleanest way to feel the difference. Imagine you tried to fix it with a sticker chart.
We're not talking about arbitrary reinforcers like giving the person something to incentivize not having a panic attack, for example. So saying to somebody, if you stop hyperventilating, I'll give you this cookie. That sounds pretty silly. We're talking about understanding how negative reinforcement functions in the context of the experience of anxiety. From the talk — Dr. Clelia Sigaud
Why does the cookie sound silly? Because the cookie is not on the same axis as the problem. The cookie is a positive reinforcer for a behavior the body is not under voluntary control of in that moment. The wave is not a choice. The escape that ends the wave is the only thing the body is offering up, and it is being negatively reinforced by the wave shutting off. If your plan adds a positive reinforcer for "stay in seat" while the wave is rising, the body will choose getting out of the wave over the sticker every single time.
This is the heart of the diagnostic fork. With plain escape, arbitrary reinforcers in a thoughtful SBT plan move the data. With anxiety, they do not. If you have a clean plan, run with fidelity, and the data is not bending at all, that is a signal worth taking seriously.
The bedside check a BCBA can run tomorrow morning#
You do not need new equipment to run this check. You need five questions and one careful pair of eyes.
- How long is recovery? Plain escape, under two minutes. Anxiety driven avoidance, ten to thirty.
- Does the kid accept an easy unrelated demand right after the behavior works? Plain escape, usually yes. Anxiety, often no.
- Does the wave precede the demand or follow it? Watch for shallow breathing, posture changes, eye darting, hand wringing in the minute before the demand hits. Plain escape almost never previews. Anxiety often does.
- Does the kid talk about the situation later in a way that suggests dread? Words like "I was scared the math was coming" or repeated questions hours later about whether math will happen tomorrow.
- Does the same trigger spread? Plain escape stays put on the worksheet. Anxiety generalizes. The pencil starts to be a problem. The chair starts to be a problem. The desk starts to be a problem.
A yes on three or more of these is not a diagnosis. It is a flag that says, the wave is in the room, and your escape plan is going to behave differently than it did on the last case.
This is also the moment to be clear about scope. A BCBA does not diagnose an anxiety disorder. A BCBA can absolutely notice an anxiety driven pattern, build an intervention that respects the mechanism, and stay in their lane while coordinating with a psychologist or prescriber. Calling it correctly is upstream of every later choice.
When your escape plan is making the anxiety stronger#
This is the part Matt admitted out loud, which is rare and worth borrowing.
We had just taken this kid through an entire escape maintained intervention and it went really well. So I applied that same strategies here and everything fell apart. From the talk — Dr. Clelia Sigaud
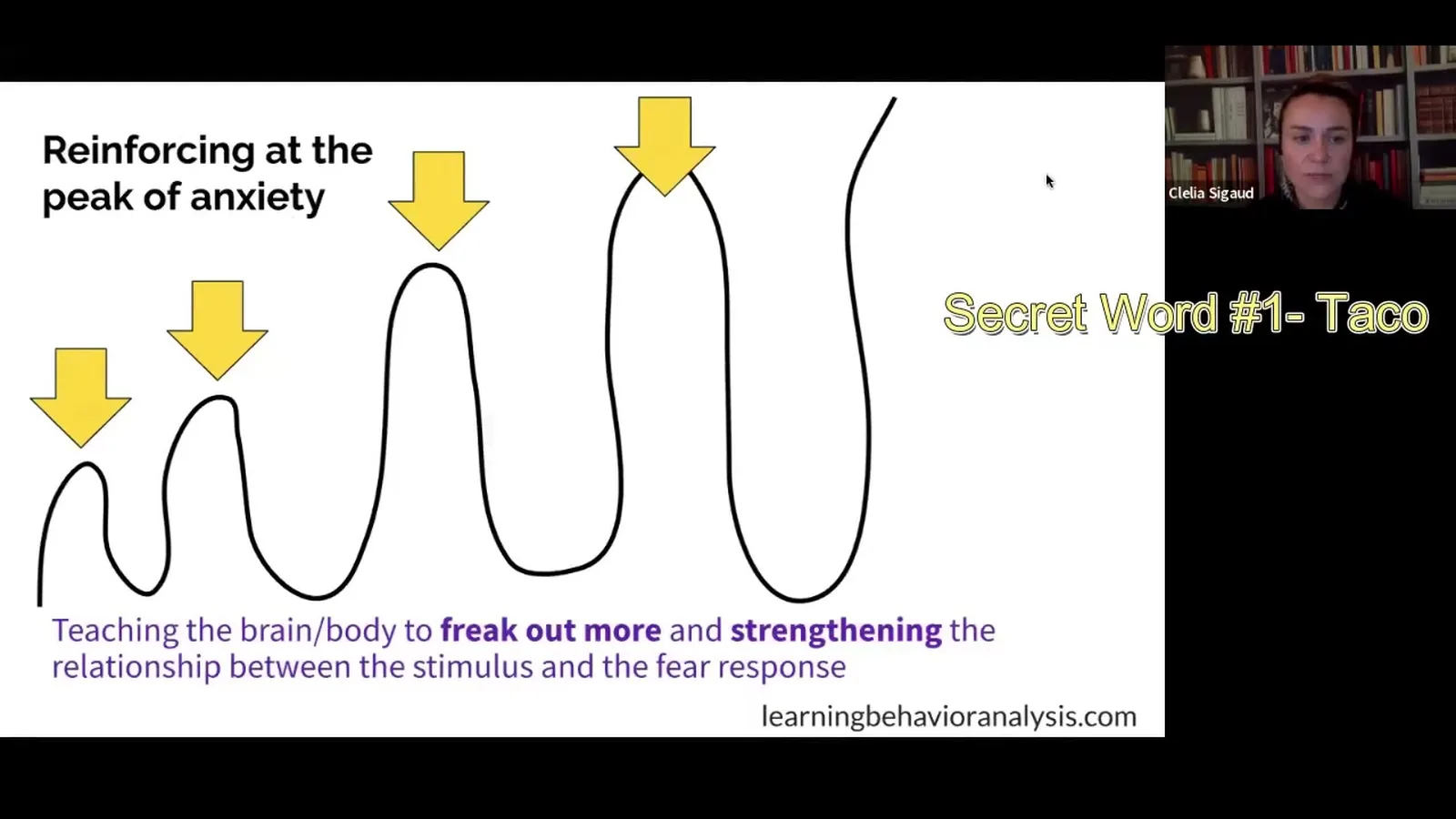
What was happening underneath. Every time the team paired the demand with a tight extinction style hold, the wave got bigger. The escape, when it finally happened, was a bigger relief. Bigger relief is bigger negative reinforcement. The next session started higher because the body had learned that this particular room, this particular adult, and this particular task were the lead in to the wave. The plan did not fail because the team ran it poorly. It failed because it was the wrong category of plan for what was actually going on.
The watch out is this. A standard escape intervention applied to anxiety driven avoidance does not just fail to help. It can teach the wave to come faster, climb higher, and hook to more cues. If you are four days in and the data is sliding the wrong way and the team's confidence is dropping, that is the cue to pause and re run the diagnostic fork, not the cue to push harder on fidelity.
How to switch lanes without scrapping the whole BIP#
You do not throw the behavior intervention plan (BIP) out. You change what the plan is treating. The skill teaching pieces, the functional communication targets, the reinforcement systems for routines outside the trigger window, all of that stays. What changes is the moment the wave starts.
In broad strokes the new lane has three pieces. First, you build a step ladder of graduated exposure that the kid actually consents to, with steps small enough that the wave never reaches the red. Second, you teach simple coping responses inside the green zone so they are available when the kid moves up a step, breathing, naming the body, asking for a break in a specific way. Third, you change what the team does in the moment the wave is rising. Instead of holding the demand and extinguishing escape, you back off to the last step where the kid was regulated, sit there for a minute, and try the next step again when the body is back in the green. That is the bones of an exposure based plan, and it is built out on the sibling pages.
When the team learns to read the wave instead of just reading the data sheet, the same kid who collapsed the first SBT plan starts moving up the ladder. The behavior numbers will not start moving for the first week or two, because you are working below the level where behavior shows up. Trust the wave shape. The numbers follow.
Frequently asked questions#
Can a kid have both escape-maintained behavior and an anxiety disorder at the same time?
Yes, and it is common. A single kid can have a plain escape pattern around one routine, like cleanup, and an anxiety driven pattern around another, like reading aloud. The BIP should call out each one separately, with its own driver, its own data, and its own plan. Treating both with one generic escape plan is the trap. Treating both with one generic anxiety plan is also the trap. Run the bedside check on each routine that shows behavior, not on the kid as a whole.
Will a standard FA pick up anxiety, or do I need a different assessment?
A standard functional analysis will tell you the behavior terminates the demand. It will not tell you why the kid needed it terminated that badly. You need to layer on antecedent observation, recovery timing, and reports from caregivers about what the kid says before and after. A trauma informed functional assessment, or a clinical interview with a psychologist for the diagnostic question, fills the gap your FA cannot fill on its own.
If anxiety is a private event, can a BCBA actually treat it?
A BCBA can build interventions that change the public conditions around the private event in ways that are well supported in the literature, graduated exposure, response prevention shaped carefully, coping skills taught in the green zone. A BCBA does not provide psychotherapy and does not diagnose. Inside scope of competence and scope of practice, there is a lot of useful, evidence based work a behavior analyst can do, especially in coordination with a psychologist or prescriber.
Watch the talk and keep going#
The fastest way to lock this in is to watch Dr. Sigaud's full session. The diagnostic fork, the cookie example, and Matt's school case play out in real time, with the kind of nuance a transcript flattens.
When you are ready for the next step, the sibling pages walk you through what to run once you have called it correctly.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Hey, Chillax Man! Understanding the Logic of Anxiety with Dr. Clelia Sigaud and earn 1.5 free BCBA CEUs. Detailed certificate, delivered the moment you finish.