How Care Collaboration Helps BCBAs Stay Inside Scope of Practice
Everything is behavior does not mean everything is yours to treat. Learn when to defer, when to refer, and how to collab, from a BCBA-led CEU.
Key takeaway
Care collaboration is the guardrail that keeps a BCBA from sliding into the "everything is behavior, so everything is mine to treat" trap, the trap that turns a BCBA into the person running a feeding program with no swallow study on file, or the person trying to teach phonics because reading is a behavior too.
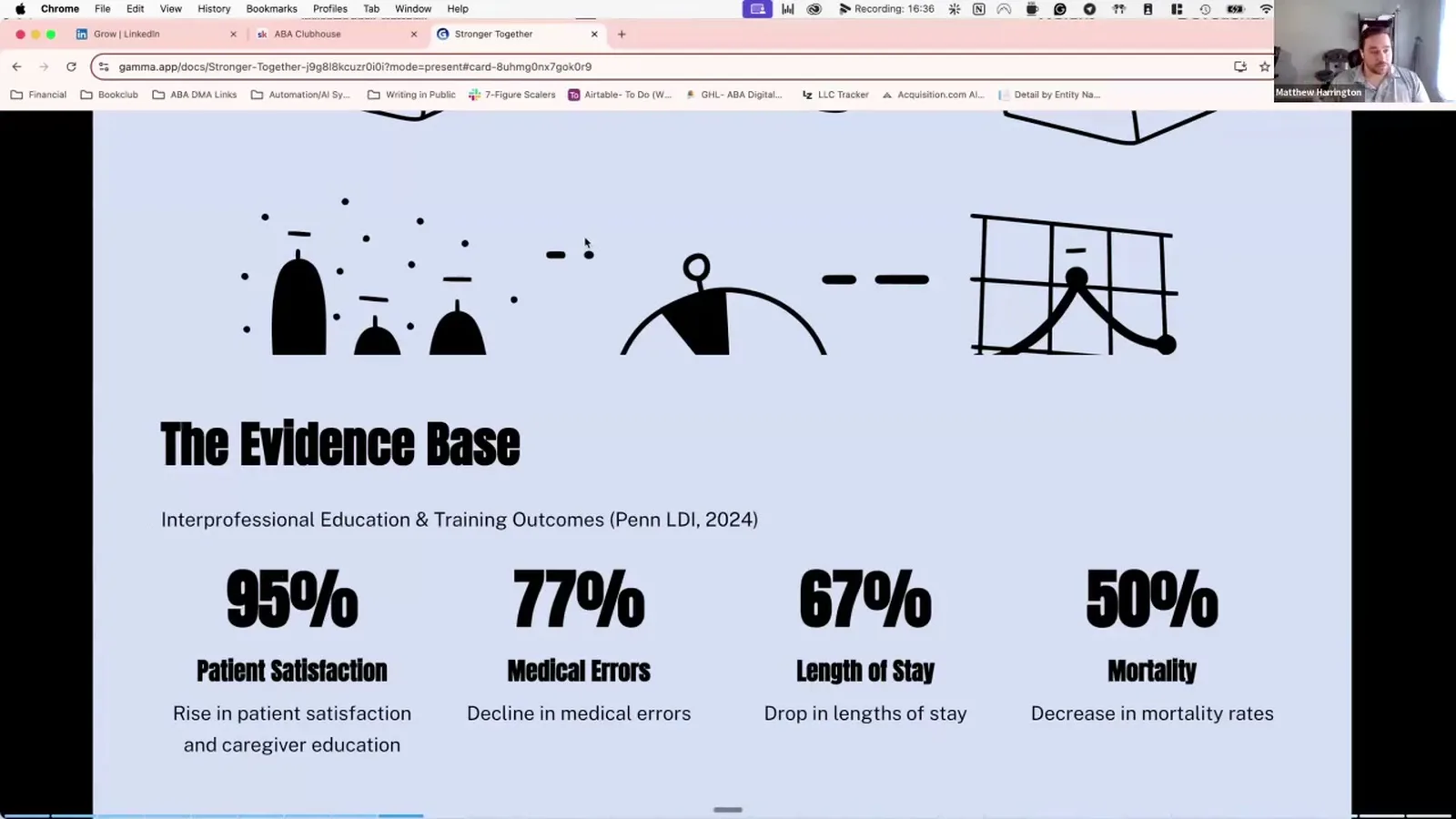
Stronger Together: Care Collab
On this page · 9 sections▾
How Care Collaboration Helps BCBAs Stay Inside Scope of Practice
Care collaboration is the guardrail that keeps a BCBA from sliding into the "everything is behavior, so everything is mine to treat" trap, the trap that turns a BCBA into the person running a feeding program with no swallow study on file, or the person trying to teach phonics because reading is a behavior too. Both of those stories show up in this CEU, one from a hospital feeding unit and one from a graduate student practicing the sound of every letter in a bedroom mirror, and both end the same way: the BCBA backs up, brings in the right professional, and ends up with a better outcome than they could have gotten alone.
What scope of practice means for a BCBA in 2026#
Scope of practice is the list of things you are trained, credentialed, and supported to treat right now, in the setting you actually work in. It is not the list of things behavior analysis can in theory address. Those two lists used to feel like the same list in grad school. They are not the same list once you have a caseload.
A BCBA who supervises severe behavior in a hospital where a feeding team is one elevator ride away has a different scope than the same BCBA two years later, working from a home office, with one part-time RBT and a Google Meet link. Same credential. Same person. Different scope, because the supports around them changed.
In 2026 the BACB still expects you to know that difference and act on it.
The everything is behavior trap#
The trap sounds smart in a grad school seminar and gets a BCBA into trouble on a real caseload. Matt names it out loud in the talk:
"Everything is behavior so we can target everything. That's true, everything is behavior, internal, external, and the science does apply. What that doesn't mean is that we are the experts in everything."
The story he uses to show what that actually feels like is small and personal. His now-wife was a special ed student doing an internship on the science of reading. She was practicing the correct sound for each letter in a mirror. He, a freshly minted RBT at the time, watched her catch herself say "buh" instead of the clean "b" sound and correct it. He realized he could have walked into a session that week and "taught" reading because reading is verbal behavior. He would have been wrong. She had three years of school and hundreds of internship hours in a method he had never opened.
That is the trap. Not malice. Not arrogance. Just the quiet assumption that a science of behavior is the same thing as expertise in every applied field that touches behavior.
Codes 1.05, 2.02, and 4.02 in plain language#
Three codes carry most of the weight here, and they read cleaner without the legal voice.
Code 1.05 says you stay inside the boundaries of what your training and experience actually cover. If a goal is on the edge of those boundaries, you do not just go for it. You get more training, you get supervision, or you refer.
Code 2.02 says you work with other providers when your client needs more than one professional at the table. It is not optional politeness. It is part of the job.
Code 4.02 says the people who pay for care and live with the outcome, usually caregivers, get to be part of the plan. They consent. They are kept in the loop. They are not handed a finished plan and asked to sign.
Read together, those three codes say the same thing: do not work alone on something that needs a team, and do not pretend the team is optional.
When your setting shrinks your scope#
This is the part most grad programs do not cover. Your scope follows your setting, and your setting can change overnight. Matt walks straight through it:
"In the hospital setting I could work with people who had swallowing issues, I could work with folks who had emesis, I could work with folks who had gagging struggles. But once I left that support... suddenly your scope of practice changes."
In the hospital, a swallow study was a phone call. An SLP was down the hall. A medical workup was already done before the feeding team ever picked up a spoon. When he moved into outpatient work without that infrastructure, the same feeding goal became unsafe. Same BCBA. Same training. Smaller scope, because the backup left the building.
The honest answer when a parent asks for a feeding program in that second setting is not "yes, here is a protocol." It is "let's get a swallow study and an SLP on this case first, then I can take on the behavioral piece." One of his real clients went exactly that route. Pediatrician first. SLP first. Then the BCBA, with the team already in place.
Saying no as the ethical answer#
A lot of BCBAs were trained to treat "no" as a failure. In scope of practice work, "no" is often the most ethical sentence in the chart note.
One participant in the live chat said it cleanly:
"I've had to shrink my scope in my career to delimiting collaboration availability."
That is not a defeat. That is a clinician noticing that without the right partners around them, certain goals stop being safe to take on. The right move is to name what you can do, name what you cannot do here, and point the family to a setting that has the missing piece. Sometimes that is a hospital. Sometimes it is an inpatient program. Sometimes it is convincing insurance to fund travel to a metro area with a specialist.
It does not feel good in the moment, especially in a rural area where the referral options are thin. It is still the right call.
Using collab to expand what you can safely treat#
Here is where collaboration stops being a chore and starts paying off. Most goals that sit just outside your solo scope move back inside scope the moment the right professional is on the case with you.
Feeding with a confirmed swallow study and an SLP partner: in scope. Feeding with no medical workup and no SLP: out of scope.
A behavior plan that touches language goals with an SLP reviewing and weighing in: in scope. The same plan written alone by a BCBA who decided to "handle the language part too": out of scope.
The way Matt frames the SLP relationship is worth keeping. Their job in collaboration is not to glance at your plan and wish you well. It is to tell you, in their professional voice, how their work and your work fit together so each one gets stronger. You ask how they taught a skill. You ask what worked in two weeks versus three months. You feed that back into your prompting and your teaching procedures. They do the same with your data.
Same for OT. His brother is a pediatric OT. The two of them have spent dinner arguments using different words for the same thing, sensory diet on one side and competing stimulus assessment on the other, both pointed at the same outcome: the kid feels safe and gets to do what they want to do. The collaboration only works once both sides agree to talk about what is actually happening for the learner instead of which vocabulary wins.
Feeding, sleep, and other gray-area examples#
A few quick reads on common gray areas.
Feeding. If there is any history of choking, gagging, emesis, or unexplained refusal, you do not start a feeding program until a medical provider has cleared swallow safety. The SLP runs swallow. The BCBA runs the behavioral piece. Both names go in the plan.
Sleep. Sleep data is some of the highest-value collaboration data you can bring to a psychiatrist. Two weeks of sleep plus behavior plus affect, graphed and lined up, can change a prescribing decision that would otherwise be made on "how have things been." That is in scope. Diagnosing a sleep disorder or recommending melatonin dose is not.
Reading and academics. Reading instruction is its own field with its own evidence base. A BCBA can run reinforcement systems around reading practice, can help with attending and on-task behavior during reading, can collect data on fluency. A BCBA does not pick the phonics method. The special ed teacher or reading specialist does.
Psychiatry. You are not adjusting medication. You are giving the psychiatrist data they cannot collect in a fifteen-minute appointment. Behavior frequency, sleep, affect, antecedent patterns. Bring the graph. Let them prescribe.
The pattern in all four: there is a behavioral seat at the table, and there is a non-behavioral seat at the table, and the BCBA stays in the behavioral seat.
FAQ#
What counts as a scope of practice violation for a BCBA? Treating a goal that requires training, credentialing, or supports you do not currently have, without a qualified partner on the case. Writing a feeding plan with no medical workup. Picking a phonics method. Adjusting medication recommendations. Diagnosing a co-occurring condition. The common thread is acting alone in a lane that needs someone else's expertise.
Does the BACB require care collaboration? Yes, when the client needs it. Code 2.02 covers professional cooperation with other providers, and code 1.05 says you stay inside your own competence, which often means bringing in someone else. It is built into the ethics code, not a nice-to-have.
How do I know when to refer instead of treat? Two questions. Do I have current training and supervised experience in this specific area? Do I have the supports I need in this setting to do it safely? If either answer is no, refer first and collaborate from there. You can still hold the behavioral piece once the right partner is on the case.
Can my scope change if I switch clinic settings? Yes, and it usually does. A move from hospital to home-based work, or from a multidisciplinary clinic to a solo practice, can shrink your scope on day one. The credential follows you. The supports do not.
What do I say when a parent wants me to treat outside my scope? Be honest and stay useful. Name what you can do, name what needs another provider, and offer to help line that provider up. Something like, "I can run the behavior piece on this once we have a swallow study and an SLP on the case. Want me to help get those started?" Parents almost always say yes when the no comes with a next step.
Keep going#
If you want the full hour with the live chat, the data slides, and the conflict resolution piece we did not cover here, the recording is on openceu.com.
Watch the full Stronger Together: Care Collab CEU
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Stronger Together: Care Collab with Matt Harrington and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.