The PDA Escalation Cycle: Why Behaviors Don't Actually Come Out of Nowhere
How to spot the engaged → delay → withdrawal → refusal → escalation sequence in a PDA profile before it tips, from a BCBA-led CEU.
Key takeaway
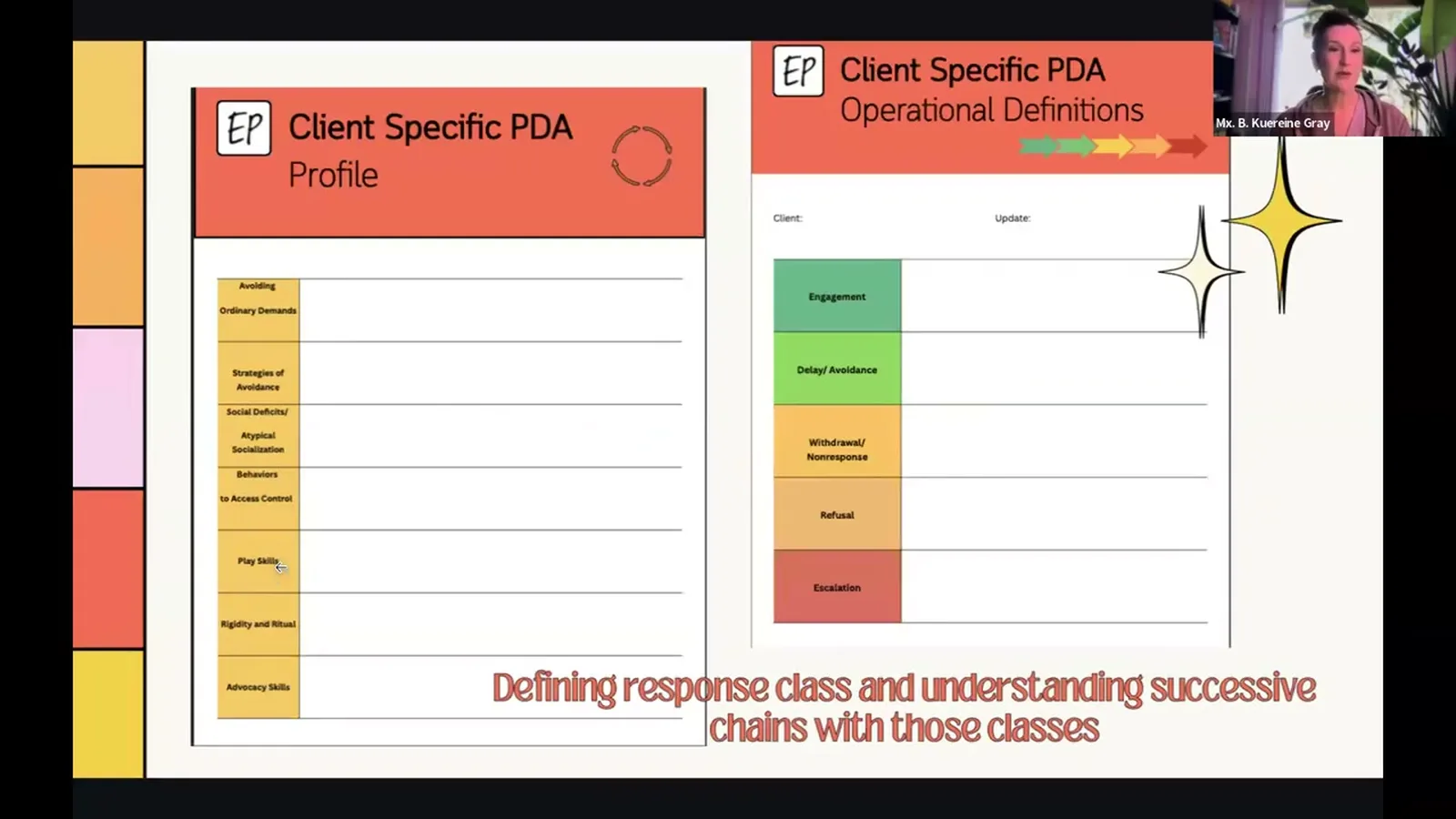
The PDA escalation cycle is a five-step chain. The steps are engaged, delay and avoidance, withdrawal and non-response, refusal, and full escalation.
PDA: Collaborating for Success
On this page · 8 sections▾
The PDA escalation cycle is a five-step chain. The steps are engaged, delay and avoidance, withdrawal and non-response, refusal, and full escalation. A learner with a PDA profile (Pathological Demand Avoidance, an autism profile) moves through these steps when a demand feels like too much for their nervous system. Most clinicians miss it because the first three steps are quiet. They can look like a calm kid, a bored kid, or a kid following along. So when aggression shows up, it feels like it came out of nowhere. This page teaches your eye to catch the chain early, name each step, and write it into a plan everyone around the learner can use.
The Short Answer: PDA Behaviors Move Through Five Predictable Phases#
The cycle runs in order: engaged, then delay and avoidance, then withdrawal and non-response, then refusal, then escalation. Each step has its own look. Each one is a chance to read what the learner's nervous system is doing. The job of the behavior stays the same the whole way through. The learner wants safety and predictability back. How they try to get it changes as the demand gets harder to hold.
This matters more than a normal antecedent (what happens right before), behavior, consequence chain. The early steps of PDA are easy to miss. A child goes still. A teen pivots to an off-topic question. An adult slowly walks away from a request. None of that looks like "behavior" the way most teams are trained to spot. Mapping the cycle makes those quiet steps easy to see. Then the team can respond at step two instead of step five.
It is many times people say, oh, the behaviors come out of nowhere. Well, we know that the behaviors don't come out of nowhere, but sometimes that sequence of escalation can be subclinical or very nuanced, and it is hard to grapple. But once we start noticing those patterns, that chain of responses that go together, and we can outline them, this will be more helpful with any other teachers, community members, caregivers, support staff.From the talk — B. Kuereine Gray
If you only take one thing from this page, take this. The cycle is real. You can write it down. And writing it down is the help everyone around the learner has been waiting for.
Phase 1. Engaged: What Baseline Actually Looks Like (and Why It's Often Masked)#
Baseline for a learner with a PDA profile rarely looks like a textbook "engaged" student. It often looks quiet. The face is flat or close to neutral. The body is still. The voice sounds normal. It can read as content, bored, shut down, or "she's just shy." All of those reads are wrong, and that is the first place the cycle gets missed.
The harder part: engagement in a PDA profile is often masked. The learner is holding it together. They are tracking and going along with the request. But that work costs them, and the cost doesn't show on the outside until they can't pay it anymore. Caregivers, teachers, and supervisors will keep telling you the kid is "fine at school" or the adult is "great at work." They are not lying. They are telling you about the mask.
It is very frequent in my experience that you see masking until the environment is unsustainable. And then you see what appears to be a big reaction out of nowhere.From the talk — B. Kuereine Gray
When you spell out this phase for your learner, write down what their real engaged baseline looks like. The face. The body. The voice. How often they start talking on their own. How fast they answer. Then write down what the masked version looks like, because that is what most people will report. Both belong on the data sheet. The gap between them is your early warning sign.
Phase 2. Delay and Avoidance: Non-Response, Active Ignoring, Off-Topic Bids#
Step two is where the chain becomes visible if you know what you are looking at. It starts with no response. The head doesn't come up. The eyes don't shift. The request lands and nothing happens. That is the first measurable drop in the learner's ability to engage with the demand.
From there it builds. Walking away. Turning the body. Picking up a different activity. Then off-topic questions. A question that sounds task-related but isn't. A sudden interest in something across the room. A comment about the weather. With many learners there is a small build inside this one step. No response moves to active ignoring, then to topic-shifting. All of it does the same job. "I am moving away from this demand without telling you I'm moving away."
When engaged, quiet, can be a blunted affect, can be a slightly neutral or even happy affect, still body... When we get into delay and avoidance, first we have non-response, which is I'm not looking up, I'm not engaging, I have ignored you. Then we would move on to more active non-response. So this child actually has an escalation within each class, which is I'm going to walk away or I'm going to start doing something different.From the talk — B. Kuereine Gray
If you map this step well, you will catch most learners here. The behavior is still low-cost for the learner and low-stakes for the room. That is when a supportive response can keep the cycle from tipping. In PFA/SBT terms (Practical Functional Assessment and Skill-Based Treatment, a common BCBA framework), this is where your R3 precursor data lives.
Phase 3. Refusal and "Socially Shocking" Behaviors That Sideline Caregivers#
By the time you are in refusal, the learner has stopped trying to slip the demand. Now they are naming it. "I don't want to." "Why do I have to?" "No." For many learners with a PDA profile, this is also where you start to hear words that are not part of how they usually talk. Swearing from a kid who doesn't swear. Name-calling from a teen who is usually careful. Lines that seem designed to shock the adult in the room.
Gray calls this "socially shocking" behavior, and it deserves its own name. The cost to the learner is small. It is one sentence. But the payoff from the room is huge. The adult freezes. They talk about the words instead of the task. They call a team meeting about the swearing. The original request quietly goes away. The learner gets what their nervous system was asking for (away from the demand, back to safe and predictable) without ever doing anything dangerous.
Good clinicians get pulled off the trail right here. The shocking words grab so much attention that they read as the problem. They aren't. They are a move inside the chain. Log them as part of refusal. Keep your eyes on the demand that pulled them out.
Phase 4. Full Escalation: Aggression, SIB, Property Destruction#
Step four is the part that gets the IEP meeting called (Individualized Education Program, the school's plan for the student). By full escalation, none of the earlier moves got the demand to go away. The learner's nervous system is out of room. This is where aggression, self-injury, and property destruction show up.
Here is the part to say out loud. By step four, the work for that episode is mostly safety and calming down. The real clinical work, the work that changes the next episode, comes from cleaner data on steps one through three. That is what lets the team break the chain earlier. If your behavior plan only logs step four (the way most plans do), your graph will make the behavior look like it really did come out of nowhere.
Here is one example from the talk. An 18-year-old had severe toileting avoidance. The family could predict big episodes from his bowel schedule. The escalation wasn't about a demand from outside. It was about a demand from inside his own body. Once the family learned the cycle, they stopped reading it as defiance. They started treating it as "he's overwhelmed." The episodes didn't go away, but the team stopped feeding them.
How to Map Your Learner's Cycle (a Worked Example)#
A useful PDA cycle map is one table per learner, built as a team. List the five steps down the side. List the learner's specific, visible behaviors across the top. You are not copying a textbook list. You are building it from FBA data (Functional Behavior Assessment, the BCBA's behavior workup), caregiver report, and your own watching.
Take Gray's eight-year-old. Engaged: quiet, slightly flat face, still body, normal voice. Delay and avoidance: head down, then walking away, then "let me ask you something else first." A small build inside one step. Refusal: "I don't want to," sometimes with a line he doesn't use anywhere else (Gray's example: an out-of-context quote from a sibling's YouTube video, used for social effect). Escalation: if the demand stays, the chain finishes.
In PFA/SBT words, the cycle lines up with something most BCBAs already use. Engaged time is your HRE window (Happy, Relaxed, and Engaged, the safe-baseline window). The delay-and-avoidance step is where your R3 precursors live. Refusal sits in your R2s. Full escalation is your R3. Putting both side by side on one page makes the map easy to share. The school team, the in-home team, and a new caregiver can all read it without a long training.
The format matters less than two things. Every behavior is spelled out exactly. And the document gets shared with everyone who works with the learner. A clean map that the sub, the bus driver, and the grandparent can all read is doing more for that learner than another goal in the treatment plan.
Why Catching the Early Phases Changes Everything Downstream#
There are two reasons to push the team's attention back to steps one and two. The first is learning history. Every episode that ends in full escalation builds a stronger link between the demand and being overwhelmed. That makes the next episode start earlier and run faster. Catching the chain at step two, and changing the demand or the room then, breaks that link before it locks in.
The second reason is teamwork. A cycle map is the most useful document for getting caregivers, teachers, and support staff on the same page. It gives non-clinicians the words for what they are seeing. It tells them what step they are in. And it tells them what not to do. Most often that means do not add pressure, do not add cheer, and do not say out loud that you can see them struggling. That last one is where well-meaning adults most often speed up the cycle by mistake.
Once the map exists, the rest of the work becomes possible. What to do at each step. How to give back some control. How to co-regulate. That is the PANDA approach, and it is a separate page. Mapping the cycle comes first. Without the map, every strategy is aimed at a step the team can't reliably see.
Frequently asked questions#
How is the PDA escalation cycle different from a typical antecedent-behavior-consequence chain?
A normal ABC chain treats each behavior as its own event with its own job. The PDA cycle treats five different-looking behaviors (silence, walking away, off-topic questions, swearing, aggression) as part of one set, doing one job: get back to safe and predictable. The cycle makes the team log the quiet, early behaviors as data. A normal ABC sheet usually throws those out. It also changes what "consequence" means. Instead of looking at what happened after the aggression, you look at what happened after the first no-response. That is where the real cause-and-effect lives.
Can the escalation cycle skip phases or move backward?
Yes, and how easily it does is useful information. Some learners run the whole chain in order every time. Others jump from step two to step four when the demand is really hard, or when they have been masking for hours. Going backward happens too. A well-timed supportive response at step three can drop the learner back to step two, or even to baseline. That is what you want to see in the data. Track direction and speed of movement for each learner. The pattern matters more than any single episode.
How long does each phase usually last before the next one starts?
There is no set timing. Treating step length as a fixed rule of PDA will lead you wrong. How long each step lasts depends on the learner's nervous system that day, how much demand has piled up earlier, the specific demand, and whether someone is co-regulating or leaving them alone. For some learners, step two can hold forty minutes. For others, the whole chain runs in ninety seconds. Measure step length per learner. Shorter steps are a warning sign. It usually means total overwhelm across the day is climbing, and the team needs to revisit supports before the next episode.
Watch the full talk: PDA: Collaborating for Success with B. Kuereine Gray. The 64-minute recording goes deeper. It covers how the clinician's own triggers show up inside the cycle, the Carlazi 2025 caregiver-implementation study, and how to use the cycle map to check if your current plan is working.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch PDA: Collaborating for Success with B. Kuereine Gray and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.