Persistent Drive for Autonomy vs. Pathological Demand Avoidance: Why the Language You Use Matters
Why more clinicians are reframing PDA as a persistent drive for autonomy, and what changes when you do, from a BCBA-led CEU.
Key takeaway
"Persistent drive for autonomy" and "pathological demand avoidance" point at the same behavior. Both names describe a kid who pushes back hard when they feel pressured.
PDA: Collaborating for Success
On this page · 7 sections▾
"Persistent drive for autonomy" and "pathological demand avoidance" point at the same behavior. Both names describe a kid who pushes back hard when they feel pressured. Fear runs the show. But the two names tell very different stories. The first name says the kid is trying to feel safe and in control. The second name says the kid is broken and avoids normal tasks. Same kid. Same actions. Two very different talks with the family and the school.
The Short Answer: Same Behavior, Two Very Different Frames#
The behaviors do not change when you swap the term. The eight-year-old still avoids the math worksheet. The eighteen-year-old still melts down around a bathroom need they cannot put off. The eleven-year-old still freezes at the busy art show. What changes is the story you tell about why. That story shapes what you try, how the parents respond, and how you feel in the room.
"Pathological demand avoidance" puts the problem inside the kid. The behavior is the disorder. "Persistent drive for autonomy" puts the problem on a need that is not being met. The behavior is the kid's best try. In behavior-analytic terms, both still point to the same job for the behavior. The kid wants control. The kid wants to feel safe. But the words you bring into the room decide if people show up open or guarded.
No longer discussing pathological demand avoidance. We're now looking at persistent drive for autonomy. Yes, when you're talking with professionals, it is important that you can use vocabulary on both sides. But when you're talking with caregivers, when you're talking with other teachers, it's really important that not only do you say, hey, this is known by the psychological community as pathological demand avoidance. I just want you to know that term. But let's look at it as a persistent drive for autonomy.From the talk — B. Kuereine Gray
Where "Pathological Demand Avoidance" Came From and What It Gets Right#
Elizabeth Newson came up with the term in the 1980s. She worked with kids whose traits did not match the autism profile of that time. Her first writeup described kids who resisted normal requests in a stubborn way. They used social tricks to avoid tasks. They seemed friendly on the surface. Their moods shifted fast. The name gave clinicians a way to talk about a pattern that normal tools kept failing on.
Where the old label still helps is the quiet warning to the BCBA (Board Certified Behavior Analyst, the clinician running the case). This is not normal escape behavior. The usual moves of slowly fading demands and gentle exposure often make things worse here. The kid reads those moves as more pressure, not less. So the term flags a group of kids where your go-to playbook will miss. That is a real win.
Where it ages badly is everywhere else. "Pathological" is a medical word. In the room, it lands like a moral one. Parents hear "your child is broken." Adults with this profile hear "the thing you do to survive is sick." Schools hear "this is the kid's fault." None of that helps the next request you are about to give.
Why "Persistent Drive for Autonomy" Is Catching On With Clinicians and Self-Advocates#
Three things are pushing the new name. The first is the adult PDA community. These are adults who live with the profile and call themselves self-advocates. They have been telling their story for a decade. They do not say "I avoid tasks because I am broken." They say something closer to "my brain reads loss of control as a threat. So I do whatever I can to take some control back." That is a drive, not a disease.
The second is new research. The Kildahl review from 2021 is the one to cite. It pushed back on the old idea that PDA kids must have advanced speech or high IQ. It treats PDA as a response pattern that can show up across many ability levels. The Carlazzi paper from late 2025 is the first US peer-reviewed article. It looks at how families feel about treatment and how parents can run the plan at home. None of that data forces a name change. But it does poke holes in the old "normal demand, broken kid" story.
The third reason is practical. If the kid acts this way to feel safe and in control, then the plan has to give back control and lower the stress. The name "persistent drive for autonomy" tells you the job of the behavior. The name "pathological demand avoidance" only tells you what it looks like from the outside. A function-first name makes the next step clear.
It is really difficult to get over a barrier of caregiver buy-in when you are pathologizing behavior. And it does set the tone for receptivity in any stakeholders that you're working with. And if you're working with someone who is able to collaborate with you in a vocal capacity, the last thing they need is for you to say that their behaviors are pathological.From the talk — B. Kuereine Gray
When to Use Each Term (Hint: It Depends on Who You Are Talking To)#
The new name does not mean you delete the old one. Use both. Use them for different jobs.
Use "pathological demand avoidance" when: you write for funders who need a known term to approve treatment. Or you write to a psychologist who used the old research to make the diagnosis. Or you note how PDA differs from autism without PDA, or from ODD (Oppositional Defiant Disorder, a different label kids sometimes get). Or you cite the Newson, Kildahl, or O'Nions research.
Use "persistent drive for autonomy" when: you introduce the idea to parents. Or you build shared words with teachers, RBTs (Registered Behavior Technicians, the staff who run sessions), and group-home aides. Or you talk with the client, especially teens and adults. Or you write the story part of a treatment plan, where you explain why the kid does what they do.
The handoff line that works is the one Gray models in the talk. Say it like this: "The clinical world calls this pathological demand avoidance. I want you to know that term. But the way I think about it, and the way we will work on it, is as a persistent drive for autonomy." That gives the parent a name they can search. It also gives them a working idea so they do not walk out feeling judged.
How the Reframe Changes Your Sessions, Notes, and Caregiver Conversations#
A few clear shifts happen once you change the words.
Your goals get sharper. "Decrease demand avoidance" becomes "increase chances for the client to pick the order of tasks in Activity X." Or "help the client tolerate uncertainty by building visuals together." The target behavior is the same. The reason you name is the real one.
Your reactive plans get more honest. When the frame is "the kid is broken," the plan tends to say "wait it out" and "do not reinforce." When the frame is "the kid needs control to feel safe," the plan has to give some control back. Choice helps. So does flexible task order, co-regulation, and small deals. Holding all the control is the very thing that started the meltdown. → see the related page on this site
Your team talks shift. New RBTs hear "this kid is pathologically avoidant." They walk in tense. They hear "this kid has a strong need for control, so we honor it when we can and gently support when we can't." They walk in curious. Watch your session data after you change the words at the team level. The shift is clear.
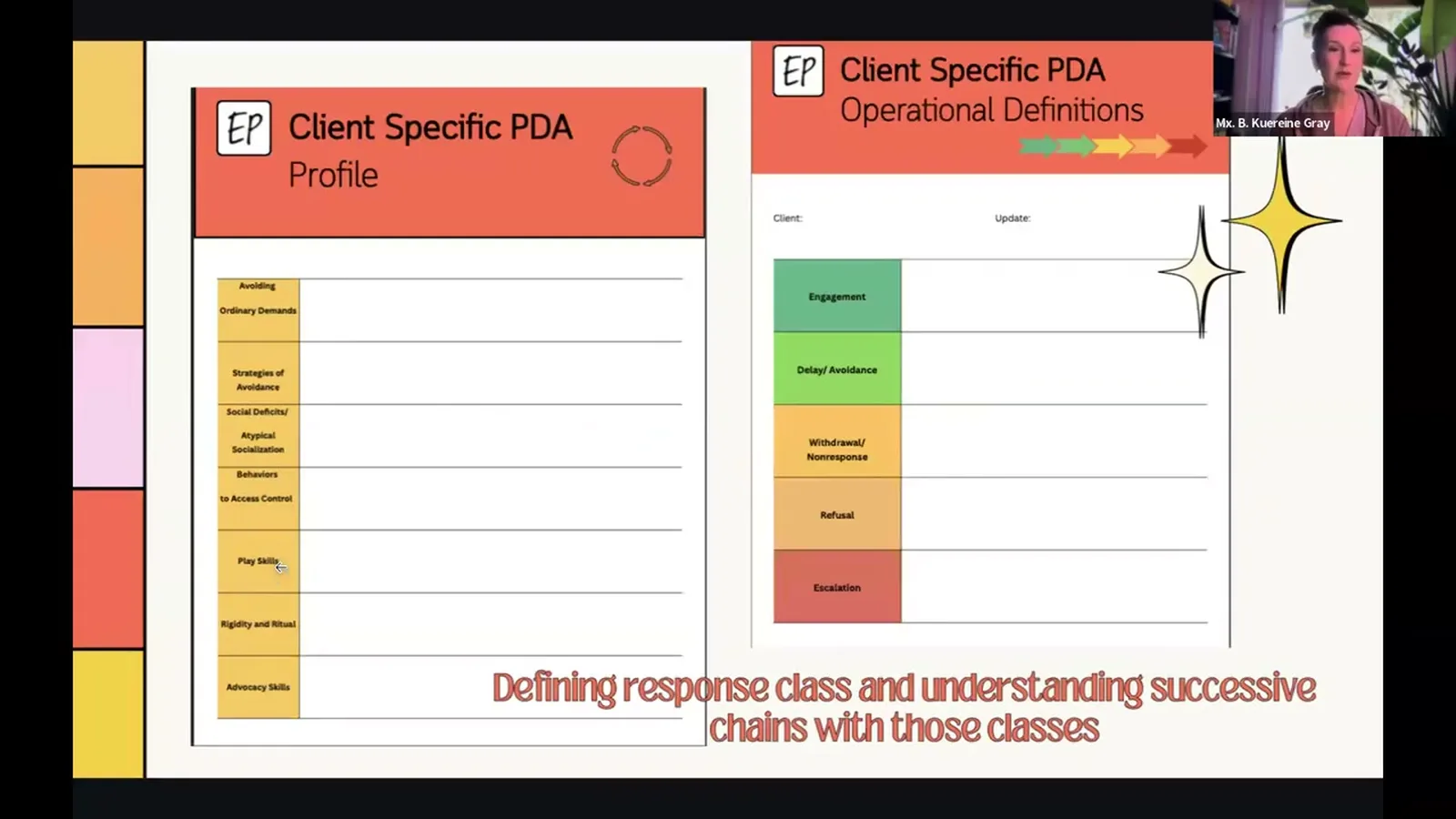
Your notes hold up under review. "Client engaged in pathological demand avoidance" is not a behavior description. It is a label said again. Try this instead. "Client used delayed echolalia and changed the topic after the request to start the worksheet. This fits the avoidance phase of the persistent-drive-for-autonomy response class." An outside reviewer can use that.
It's like your brain is split in two. There's part, there is a part which is forcing your body into shutdown and the other part is telling you, oh my God, what are you doing? You feel guilty for the parent or the teacher and it's not you that's choosing this. Your brain's trying to protect you from a threat that isn't there. Even picking up a pencil can feel like a threat. PDA rarely happens because the demand is hard, but your brain tricks you into thinking it's really hard.From the talk — B. Kuereine Gray
That voice is a teen from PAST in the UK, not a clinician. It is the clearest case in the talk for why "pathological" is the wrong word. The kid does not feel like they are choosing to avoid. They feel like they are being protected from a danger that is not real. "Persistent drive for autonomy" honors that inside view. "Pathological demand avoidance" talks over it.
Scripts: Saying the Same Thing Without Treating the Kid Like a Disease#
These are lines to keep handy. They are for the moment in session, mid-meltdown, or on a parent call. Use them when you need to name what is happening without making it worse.
In session, when you see warning signs, to the client:
"I can see you really want a say in how this goes. Let's figure out what's yours to pick and what's mine to pick."
In session, to a calm caregiver:
"He's not refusing the worksheet because the worksheet is hard. He's refusing because right now everything that gets handed to him feels like a threat to his control. We're going to give some control back, then come back to the worksheet."
On the intake call, when a parent asks what PDA is:
"The clinical term you'll see online is pathological demand avoidance. The way I think about it, and the way we'll work on it, is as a persistent drive for autonomy. His brain reads loss of control as a real threat. The behaviors you're describing are the strategies he's using to feel safe."
Writing in a treatment plan:
"Response class marked by a persistent drive for autonomy (also called pathological demand avoidance in the literature, Newson, 2003; Kildahl et al., 2021). The behavior likely works to get control and to feel safe when things feel uncertain."
To a school team that pushes back:
"I'm not asking you to drop demands. I'm asking you to share the sequencing. Same instructional content, the student picks the order."
Notice what these scripts do not do. They do not promise the kid will not melt down. They do not blame the parent. They do not ask anyone to throw out the research. They just move the cause from "this child is broken" to "this child is using the tools their brain has. We can help meet that need a better way."
Frequently asked questions#
Is "persistent drive for autonomy" a formal diagnostic term?
No. Neither name is a formal diagnosis. PDA does not have its own ICD-10 code. It is not in the DSM-5 (the main book doctors use to name conditions). "Pathological demand avoidance" has the longer research trail. You will find it in studies from the UK and, more recently, the US. "Persistent drive for autonomy" is a new way to describe it. Self-advocates and parent-facing materials use it more and more. Treat them as two names for the same pattern. The second name describes the job of the behavior. The first name describes the look of it.
Will insurance funders accept "persistent drive for autonomy" language in treatment plans?
Mixed answer. Funders approve based on the main diagnosis (usually autism) and the medical need story. They do not approve based on the PDA label itself. Lead with the main diagnosis and the behaviors you see. Note the response class with both names ("persistent drive for autonomy, also known as pathological demand avoidance, Newson 2003"). Tie your treatments to standard codes. The new name is for the people in the room. The paperwork still has to translate.
How do I explain the reframe to a parent who already uses "pathological demand avoidance"?
Do not correct them. Do not make it a vocab lesson. First, honor the term they brought in. Then add yours as the working idea. Try this. "That's the term most of the research uses, and it's a useful one for searching the literature. The way I'm going to talk about it in our sessions is as a persistent drive for autonomy, because it points us at what we're actually going to do. We give him back some control and lower the stress he's reacting to." Most parents come around to the new name in a few weeks once they see calmer sessions.
Watch the full talk. Gray walks through the response-class framework, the PANDA strategies (her five-part support plan), and parent-facing examples this article only points at. That includes the co-regulation moves she used with the eighteen-year-old and with the eleven-year-old at the art show. She also shows how the change in words paid off in those families' daily lives.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch PDA: Collaborating for Success with B. Kuereine Gray and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.