How to Talk to Parents About a PDA Profile Without Losing Buy-In
Scripts and framing for raising PDA with caregivers. What to say, what to avoid, and why word choice matters. From a BCBA-led CEU.
Key takeaway
Start with what the parent is already living with. The toilet standoffs. The "out of nowhere" meltdowns at the art exhibit. The kid who can solve a math problem one minute and refuse the worksheet the next.
PDA: Collaborating for Success
On this page · 9 sections▾
Start with what the parent is already living with. The toilet standoffs. The "out of nowhere" meltdowns at the art exhibit. The kid who can solve a math problem one minute and refuse the worksheet the next. If you open with "I think your child has a PDA profile," you've lost the room. The parent hears one of two things. Another label to chase. Or a nicer way of saying their kid is just being difficult. This page is about the order of that conversation. What you describe first. What words you use, and when. When to bring in the research. And what to do when the parent has already been told it's their fault.
The Short Answer: Lead With What They're Already Seeing, Not the Label#
Open with a behavior the parent has already told you about. Use their own words. Not "demand avoidance." Not "rigidity." Not "response class." Whatever they said on intake. "She won't put her shoes on even though she asked to go." "He holds it until he's screaming and then nothing calms him down." "She can do the math but she refuses the worksheet." Say that back. Then name the pattern, not the term.
Try this opener:
"I want to walk you through something I've been noticing in our last few sessions. When [child] is asked to do something, even something they want to do, a whole cycle happens before the outburst at the end. A lot of what feels 'out of nowhere' actually starts about ten minutes earlier. I want to show you what I'm seeing."
You haven't used the word PDA. You haven't given them a label to Google at 11pm. You've given them an answer to the part they care about most. Why their week feels unpredictable. The label comes later. Sometimes weeks later. And only after they've watched you guess their kid's behavior right twice. Trust you've earned is the currency you spend on the harder words.
The Conversation You're Trying NOT to Have (and Why It Keeps Happening)#
The conversation you don't want is the one where the parent leaves quieter than they came in. They nod at everything. Then they never reply to the follow-up email. That means you've lost them. It almost always happens because somewhere in the first ten minutes, you used a word that sounded like judgment.
"Pathological" is the obvious one. But it's not the only one. "Avoidance" sounds like a choice. "Manipulative," even in the clinical sense, lands hard with a parent who's been told for three years that their kid is "playing them." "Refusal" sounds like the kid is just being bad. Even "demand avoidance" as a phrase makes parents flinch. They hear a description of bad behavior, not a description of a nervous system.
It is really difficult to get over a barrier of caregiver buy-in when you are pathologizing behavior. And it does set the tone for receptivity in any stakeholders that you're working with. From the talk — B. Kuereine Gray
This is the main rule. Words that label the kid as sick don't just hurt feelings. They shut the door before the talk even starts. The parent stops asking questions. The follow-through dies. You can have the best plan in the world and watch it fall apart in a kitchen on a Tuesday night, because the words you sent home with the parent were the wrong words.
What to Say First: A Three-Line Opening Script#
Three lines. In order. Say them in your own voice, but keep the order.
Line 1. Reflect a specific behavior they've described:
"You told me last week that bedtime has been ending in a meltdown almost every night, even when [child] has had a really good day."
Line 2. Name the pattern, not the term:
"What I'm noticing is that the meltdown isn't really about bedtime. There's a whole sequence that starts earlier. You can see [child] start to shut down, get quiet, change the subject, get really chatty about something else. By the time we get to the actual bedtime ask, they're already partway up the escalation."
Line 3. Invite them in as the observer, not the patient:
"I want to map this out with you. You see things at home I'll never see in session. If we can spot the early signals together, the goal is fewer surprise meltdowns. For both of us."
That's it. No diagnosis. No research article. No "have you heard of PDA?" The parent walks away with two things. A sentence they can repeat to the other parent. And a job. You've made them a partner in watching, which is the role they were already playing. They just didn't have a frame for it.
How to Introduce "Persistent Drive for Autonomy" Without Losing Your Clinical Credibility#
At some point you'll need to give the pattern a name. The instinct is to say "this is called Pathological Demand Avoidance." Partly because it's the term in the literature. Partly because fancy clinical words feel like they give you credibility. They do the opposite with parents.
Use "persistent drive for autonomy" with families, teachers, and the kid. Save the clinical term for charts, supervision, and talks with other licensed providers who need to find the same research you're reading. The reframe isn't dishonest. It's matched to who you're talking to. If a parent later asks, "Why didn't you just call it pathological demand avoidance?" the answer is simple. "Because what I'm describing is your kid's brain working really hard to feel safe in a world where almost everything feels like a demand. Calling that 'pathological' would be right by the book, and useless in the kitchen. The word would make you stop hearing me."
That last line is the one I want you to actually use. It's honest about the word choice. It respects the parent. And it puts you on the same side of the table.
(For the longer breakdown of why this reframe holds up clinically, and what the literature says about both terms, see → see the related page on this site. This page stays focused on the parent talk. Your own internal language is a separate call.)
When to Bring Up Research vs. When to Just Listen#
The pull, especially with eager parents, is to lead with the research. Don't. Most parents don't need a citation in the first meeting. They need to feel like the person across from them has met their actual kid. Bring the research in the second or third talk. And only when one of two things has happened. One: the parent has asked, "Is there anything written about this?" Two: the other parent, a grandparent, or a teacher is the one who isn't on board, and the parent has asked you for ammo.
When that moment comes, hand them the Carlazi 2025 article on caregiver-implemented intervention and social validity. It's recent. It's peer-reviewed. It's free to read. And it's about whether caregivers themselves saw the plan work. That's exactly what the other parent who isn't sold yet wants to know.
There is, and it's early release, and it is free access... In March of this year, there is a peer-reviewed research article being published... it looks not at, is the intervention efficacious, but caregivers implementing the intervention and the social validity. Did they see it make an impact? From the talk — B. Kuereine Gray
Hand the parent the actual PDF. Don't summarize it for them. Don't email a link they have to click. Print it or AirDrop it. Friction kills follow-through. A parent who reads the abstract before the next session shows up ten times more bought in than one who took your word for it.
Before that moment? Listen. Ask the parent to tell you what happened the last three times the cycle blew up. Then resist the urge to interpret out loud. Most parents have never had quiet space to describe their child to someone who knows what to listen for. Your read-out can wait.
What to Do When a Parent Has Already Been Told It's "Bad Parenting"#
A lot of these parents are not first-timers. They've already been told by a teacher, a pediatrician, or their mother-in-law that the problem is them. That they're inconsistent. That they need stricter limits. That they're too soft, too anxious, too easy on the kid.
A lot of them state, oh, I'm told that it's bad parenting or I just don't have expectations or, um, it's the, uh, the full circle to the fridge mom... Something about new and scary that pushes us back into old stereotypes. From the talk — B. Kuereine Gray
If you don't bring this up, the parent will assume you think it too. Because everyone else has. So name it. Not with sympathy. With a clinical fact.
Try this:
"Before I go any further, I want to say something. I've worked with kids whose pattern looks like [child]'s. The strictest parents in the world don't change this. And the most permissive parents in the world don't cause it. The pattern shows up across families, parenting styles, and cultures. So whatever you've been told about this being a discipline problem, set it down for an hour and just listen to what I'm describing. We can come back to the parenting question if you want, but it's not where I'd start."
That short script does three jobs. It names the elephant. It rules out the thing they've been blamed for. And it lets them stop trying to look like a perfect parent for you. The shoulders come down. Then you can actually work.
Follow-Up: What Caregiver Training Actually Looks Like Week to Week#
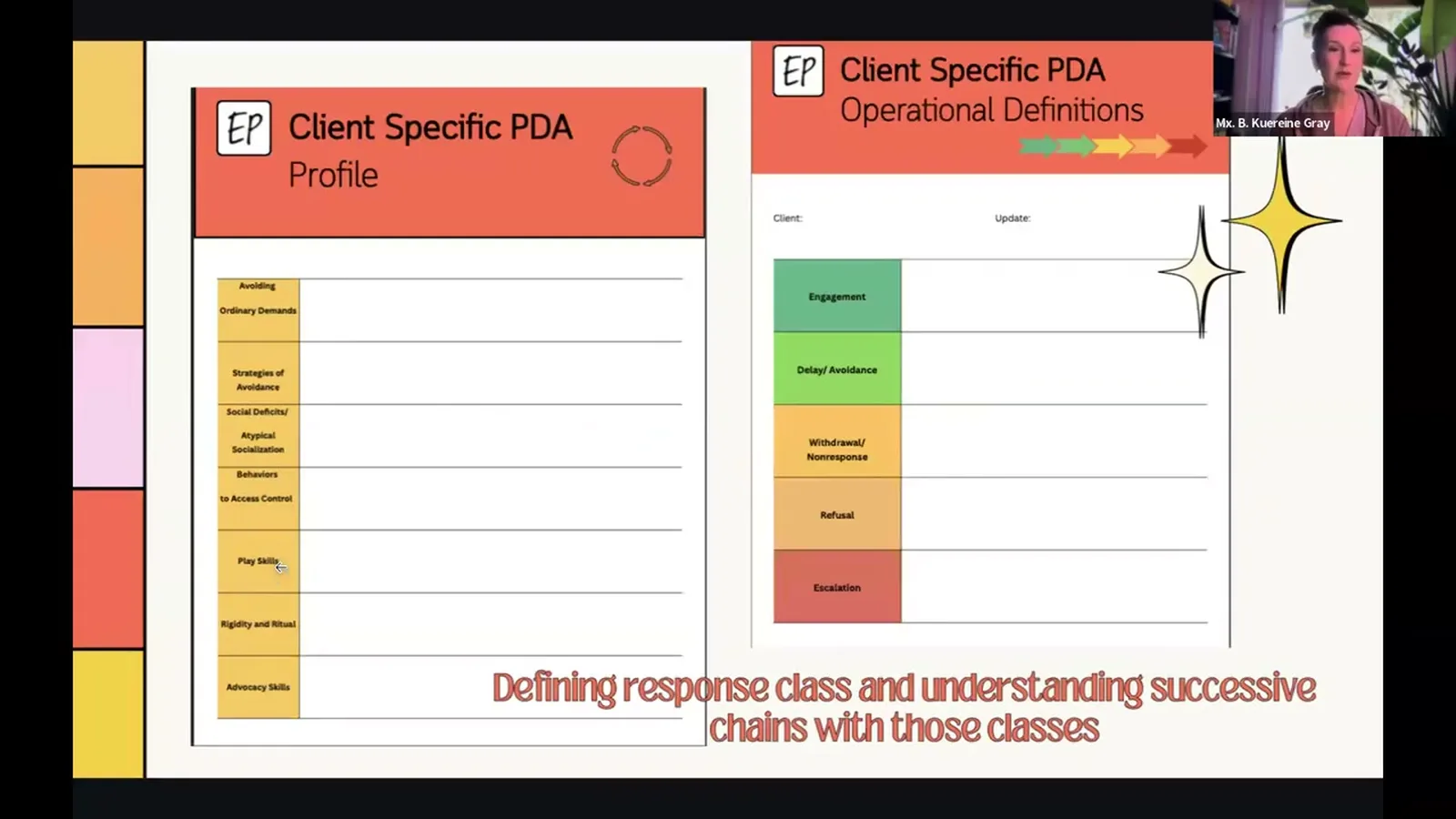
The first talk is the gate. The follow-up is where the buy-in grows or fades. Here's how. The next three to four sessions should teach the parent to spot the escalation cycle in their own footage or memory. Engaged, delay, withdrawal, refusal, escalation. Teach them to see it before you teach a single strategy. The order matters. Hand a parent a strategy before they can see the cycle, and it becomes "a trick that didn't work."
They started being able to see the full escalation cycle, with caregiver training on that escalation cycle. It allowed them to be much more supportive, as opposed to coming at the behavior and responding to him as a, oh, you just have to get over it. Go to the bathroom, man. It'll be fine. That doesn't help. From the talk — B. Kuereine Gray
That clip is the whole game. Before the parent could see the cycle, "go to the bathroom, man, it'll be fine" felt like a normal thing to say to a kid avoiding the toilet. After they could see the cycle, the same words read like gasoline. Nothing about the kid changed. The parent's read of where they were in the sequence did.
Here's a simple week-by-week. Session 1, you describe the cycle. Ask them to journal three behavior episodes in the next seven days. In writing. Without interpreting. Session 2, you read the journal entries with them. Mark where the escalation actually started. Almost always earlier than they thought. Session 3, you teach one low-arousal response they can practice in the early-delay window. Just one. Don't dump five strategies on them. The whole point is to lower demand load. That includes the load you're putting on the parent.
(If you want a walkthrough of the in-session strategies, Pick your battles, Anxiety management, Negotiation and collaboration, Disguise and manage demands, Adaptation, see → see the related page on this site.)
Frequently asked questions#
Should I bring up PDA before a formal evaluation has been done?
You can describe the pattern and use working language with the family without making a diagnosis. What you should not do is say "I think your child has PDA" as if it were a diagnosis you can give. PDA isn't a DSM category. It doesn't have an ICD code. And BCBAs (board certified behavior analysts) don't diagnose anyway. What you can ethically say: "I'm seeing a pattern that's been written about in the research. It changes how I'd run our program. I'm going to describe it. If it lines up with what you're seeing, I'd also recommend a talk with [child]'s psychologist or developmental pediatrician about whether a fuller evaluation is worth doing."
What do I do if the other parent or a co-caregiver disagrees that this is PDA?
Stop trying to win over the one who isn't on board. Start collecting data with the parent who is. Most of the time, the second parent isn't fighting the pattern. They're fighting the label, or the idea that their kid has "another thing wrong." Drop the label with that person. Ask them to track one specific behavior for two weeks. When the pattern shows up exactly when you said it would, you've earned a second talk. If they're still opposed after seeing their own data, that's a family issue, not a clinical one. Your job is to make the plan work where you do have buy-in, without becoming a wedge between the parents.
How do I document a PDA conversation in clinical notes when it isn't a formal diagnosis?
Document by behavior and description. "Discussed observed response pattern. Escalation in response to perceived demands. Subtle precursors (non-response, off-topic conversation, social negotiation) preceded overt refusal and escalation. Discussed caregiver training on response-cycle identification and proactive antecedent strategies." That's a solid note. It says what you saw, what you taught, and what the plan is. It doesn't claim a diagnosis you're not credentialed to give. If you want to point to the research, "consistent with patterns described in the PDA literature (see Kildahl, 2021; Carlazi, 2025)" is fine in a treatment plan.
Watch the full talk#
The full 60-minute talk goes deeper into the escalation cycle, the five-stage response class, and the PANDA framework for in-session work. It also has the longer caregiver-training piece this page condenses, including the clinical examples (the 18-year-old, the 8-year-old with the YouTube quote, the 11-year-old at the art exhibit) that make the framework click in a way bullet points can't. Watch the full talk →
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch PDA: Collaborating for Success with B. Kuereine Gray and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.