Parent Consent for Behavior Reduction: What Counts, What Does Not
When the consent form on file is not enough, how to do continuous informed consent, and the assent layer underneath, from a BCBA-led CEU.
Key takeaway
Every time a BCBA files a 5-5 code to change a behavior reduction plan, that is the trigger to refresh parent consent, and the potty-training case study below is the reason why: a goal can look like a win on the data sheet while quietly breaking the second-order things that made therapy worth showing up for.
Ethical Guardrails in Behavior Reduction
On this page · 8 sections▾
Every time a BCBA files a 5-5 code to change a behavior reduction plan, that is the trigger to refresh parent consent, and the potty-training case study below is the reason why: a goal can look like a win on the data sheet while quietly breaking the second-order things that made therapy worth showing up for. Parents have a right to know what is changing, why it is changing, and what else might change because of it.
What the intake consent form does and does not cover#
The consent form a caregiver signs at intake is a legal floor, not a clinical ceiling. It says the family agrees to receive ABA, agrees to the broad strokes of the assessment, and agrees to the general types of procedures you might use. What it does not do is hand you a blank check for every plan revision you write over the next two years.
Think of intake consent the way you think about a pediatrician explaining a vaccine. The parent hears the benefits, hears the risks, and signs the paper one time. That works for a single shot. It does not work for a behavior plan that gets edited every few weeks. The form on file is the starting point of an ongoing conversation, not the end of it.
If the only time you talk to a parent about consent is during initial paperwork and during the yearly reauth, you are operating on a hospital model in a setting that looks nothing like a hospital. The clinical reality is that plans change, kids change, and what a parent agreed to in March may not be what is actually happening in July.
Explaining, demonstrating, and talking to both the client and the caregiver as you are working through a behavioral intervention is crucial, not just at the very beginning, like we see in the hospital setting, but continuously. From the talk — Matt Harrington
The 5-5 trigger: when a plan change requires fresh consent#
Here is the simplest rule to put in place tomorrow. Every time you file a 5-5 code, treat it as a consent refresh event. The 5-5 code is the BACB billing code for behavior plan modification, and the BACB Ethics Code already obligates you to keep caregivers informed about the services they are receiving. Pairing those two facts gives you a clean, repeatable trigger.
A 5-5 does not always mean signing a new piece of paper. It means a real conversation: what is changing, why you are changing it, what you expect to happen, what could go sideways, and what choice the family has. That conversation can live in a parent training note, in a follow-up email, or in a quick recorded huddle. The format is yours. The duty is fixed.
This is the bridge between paperwork and the actual ethical requirement. Re-signing a form for every shaping step adjustment is theater. Walking the caregiver through a real change in approach, in language they understand, is consent.
Our interventions change frequently when we are doing our 5-5 codes. That means that each time interventions change, there should be informed consent being provided again. That does not mean that we have to re-sign a piece of paper every single time we make a small change, but that does mean continuous information being fed to all parties. From the talk — Matt Harrington
Second-order effects parents have a right to be told about#
When clinicians describe a plan to a parent, they tend to describe the target. The mand will go up. The aggression will go down. Toileting will generalize. Those are first-order effects. They are the thing on the graph.
Second-order effects are everything else the plan touches. The reinforcers you pulled. The routines you traded away. How the child feels about coming to clinic. The way the parent now talks about ABA at home. None of that lives on the target graph, but all of it lives in the family's actual experience.
Parents have a right to be told what could shift outside the target. If you are going to thin reinforcement, name it. If you are going to remove a preferred activity to make room for a new demand, name it. If you are going to make sessions harder before they get easier, name it. The point is not to scare anyone. The point is to make sure the family is choosing the trade with their eyes open.
This is also a fidelity check on you. If you cannot list the second-order effects of your plan in plain words, you do not understand your plan well enough to ask anyone to consent to it.
The case study: when "progress on the goal" hid the real story#
The clearest version of this from the talk was a potty-training case. The kid was four. Goals stack looked normal: language, transitions, light challenging behavior, no self-injury. The team ran fixed-schedule toileting, and the data was clean. Independents were going up. Generalization to home was happening. By every measure on the protocol, the plan was a win.
Then a parent training session reframed everything.
Then I stepped into parent training one day and the caregiver was like, oh my gosh, what is going on at ABA? And I was like, what do you mean? And she was like, he does not like coming anymore. He used to jump out of the car. He used to run to you. From the talk — Matt Harrington
The kid who used to jump out of the car now did not want to come in. The kid who used to talk a lot was talking less. The goal sheet had nothing to say about any of that. The plan had quietly eaten the natural reinforcers that made the clinic the place he wanted to be.
By working through this, we realized that while potty training was going great, we had taken away a lot of the reinforcers that were naturally occurring to make ABA something he actually wanted to go to. That error that I made there was that I was looking at a singular data point for a singular intervention. From the talk — Matt Harrington
The parent had consented to a potty-training plan. She had not consented to losing the version of her kid who ran into the clinic. Those are not the same agreement.
What continuous consent looks like in week-to-week practice#
Continuous consent is not a binder. It is a small set of habits.
First, every 5-5 gets a real conversation. Not a copied-and-pasted plan summary. A short, specific, plain-language walkthrough of what is changing and what to watch for at home. Five minutes, documented, done.
Second, the parent gets a heads-up on what could change outside the target. Sleep. Mood. How the kid talks about ABA. Whether transitions get harder before they get easier. If you can predict it, name it. If you cannot predict it, say that too.
Third, you build a back-channel. A weekly text. A standing 10-minute parent training slot. A note in the home log book. Whatever fits the family. The point is that the parent has a low-friction way to flag something off without waiting for the next review.
Fourth, you watch your caseload, not just your client. If you have twenty active behavior reduction targets across one kid, you cannot analyze any of them deeply enough to keep continuous consent honest. Cut to the two or three that move quality of life. Track the rest as secondary. A caregiver cannot consent to a plan no one has time to understand.
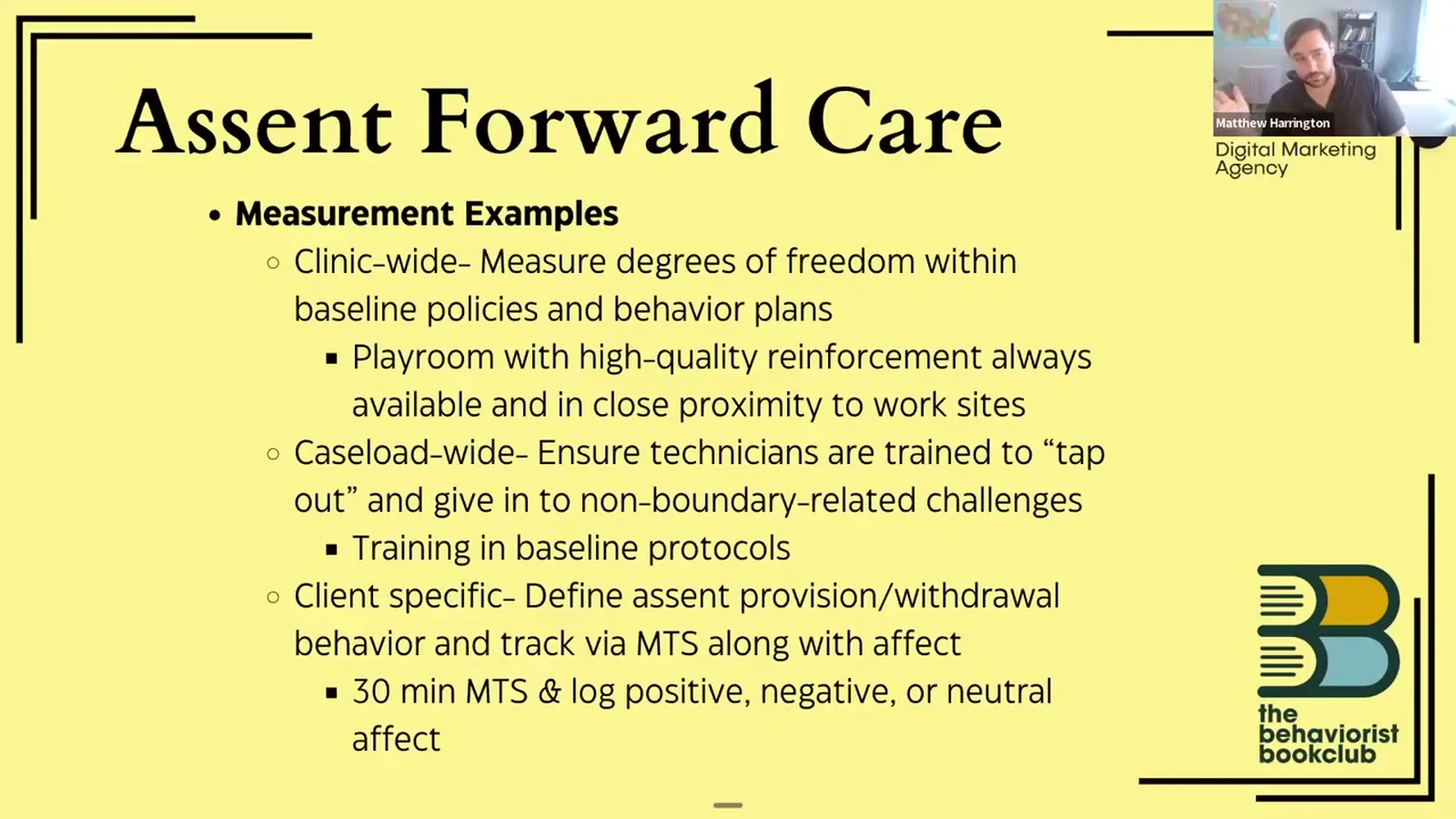
Fifth, you measure assent on the client side at the same time. Momentary time sampling every 15 or 30 minutes works. Walking toward the table, reaching for materials, body oriented to the tech, those are assent provision behaviors. Replace any of those with the opposite and you have assent withdrawal. That data is part of what you bring back to the parent.
When a parent's consent and the client's assent disagree#
Parents can consent. Clients assent. They are different signals and they will not always line up. A parent can sign off on a plan in good faith while the kid is sending you very clear non-assent the moment you start running it.
When that happens, the parent's consent does not override the client's assent. It is also not your cue to torch the plan that afternoon. It is your cue to go back to the family, share what you are seeing on the assent side, and decide together what to change. That conversation is also a 5-5 trigger. New information, new plan, fresh consent.
The opposite case matters too. A parent can pull consent for something the client is happily engaging with. Same drill: take it back to the family, share what you are seeing, and make the call together.
The pattern is the same in both directions. New data shows up, you bring it to the people who have a right to weigh in, and you do not run a plan that one party has stopped agreeing to.
Frequently asked questions#
Does my BACB consent form cover changes to the behavior plan?
Not really. The intake form covers the existence of services and the general approach. Any meaningful change to a behavior reduction plan, including anything that triggers a 5-5 code, calls for a fresh, documented conversation with the caregiver. You usually do not need a new signature. You do need a record that the conversation happened and that the family agreed to the change.
Can a parent consent to a procedure the client clearly does not assent to?
A parent can sign off on a plan that the client is not assenting to, but that is not the end of the ethical analysis, it is the start of it. Your job is to bring the assent data back to the family, explain what it means, and decide together whether to keep going, modify, or pause. A parent's consent does not erase a client's non-assent. It just means you have a harder conversation to have.
How often should I re-discuss the behavior plan with caregivers?
The honest answer is: every time the plan changes in a way you would file a 5-5 for, plus a standing weekly or biweekly touchpoint that is short and low-friction. Yearly reauth is way too slow. Every session is too much for most families. Tie it to the clinical trigger you already have to track.
Keep going#
If this is the part of the work you want to get sharper on, watch the full talk. The consent and assent material sits inside a wider framework of ethical guardrails for behavior reduction, including the second-order-effects lens that the potty-training case study cracked open.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Ethical Guardrails in Behavior Reduction with Matt Harrington and earn a free BCBA CEU. Detailed certificate, delivered the moment you finish.