Can BCBAs Bill for Care Collaboration? CPT Codes, Payer Rules, and ROI
Care collab is billable in some states and not others. Learn what to check with your payer and why it still pays off, from a BCBA-led CEU.
Key takeaway
Yes, there is a CPT code for care collaboration in some states (Virginia telehealth lets a BCBA bill about one to one and a half hours per month), but in other states like Florida it is not a billable code at all, so the real question is how to capture the return on investment when the work is unpaid.
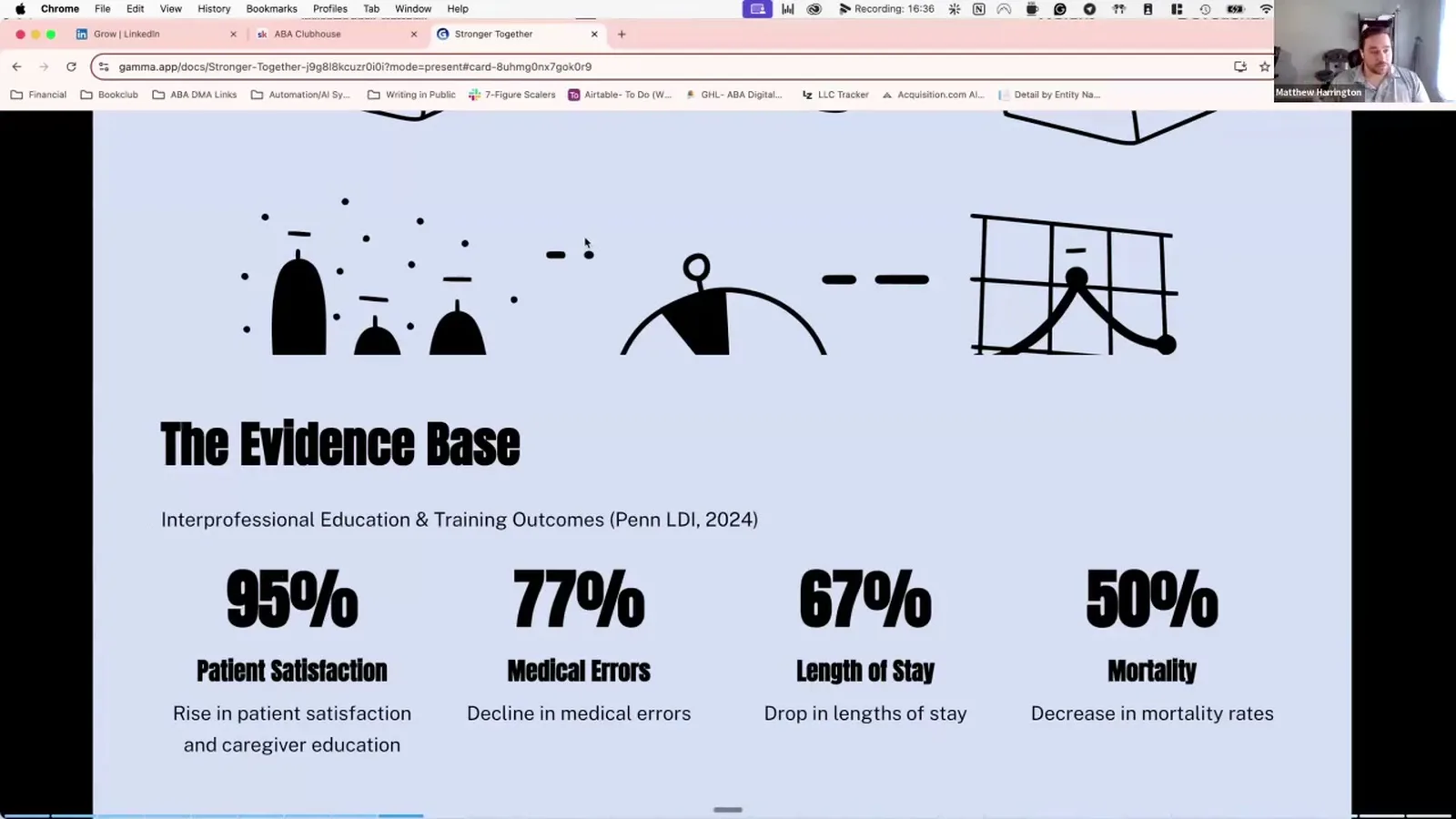
Stronger Together: Care Collab
On this page · 9 sections▾
Yes, there is a CPT code for care collaboration in some states (Virginia telehealth lets a BCBA bill about one to one and a half hours per month), but in other states like Florida it is not a billable code at all, so the real question is how to capture the return on investment when the work is unpaid. This guide walks through what the BACB recognizes, why payer rules shift, what to ask your payer before you bill, and how to prove the value of collab time even when no CPT code applies.
Is care collaboration billable for BCBAs?#
Sometimes. The answer is not a clean yes or no, and that is the part that trips up most BCBAs and clinic directors. Whether you can bill an SLP meeting, a school IEP touchpoint, or a 30 minute call with a pediatrician comes down to two things: your state, and your specific payer contract. The same BCBA who could bill collab in one job may not be able to bill it in the next.
In the recording, Matt put it plainly when an attendee asked about billing a care collaboration meeting:
Depending on your payer there's a CPT code for billing, yes.
That word "depending" is doing a lot of work. The CPT system has codes that can fit care collaboration, but each payer decides whether to recognize them, how to reimburse them, and how many hours per month they will cover. Two BCBAs at the same company can have different answers for two clients because the payers are different.
If you want a clean answer, you have to ask one client, one payer, one code at a time. There is no shortcut.
Why payer rules change state by state#
State variation is the part that surprises new BCBAs the most. You can move across a state line and lose access to a code you used every month. Matt described his own experience:
In Virginia, working telehealth, we had a code that we could bill for. I think it was like one to one and a half hours of care collaboration per month.
That worked because the Virginia plan he was billing under accepted the code and set a monthly cap. Move the same BCBA to Florida and the picture changes:
In Florida, where I am right now, you can't bill care collaboration. It's not a billable CPT code.
Why the gap? A few reasons. State Medicaid programs write their own ABA benefit rules, so what Virginia Medicaid covers may not match Florida Medicaid. Commercial plans inside a state often mirror the Medicaid lead. Some states require BCBAs to document collaboration as a quality measure but do not pay for the time. And some payers fold collaboration into the rate they already pay for direct treatment, which is why they will not pay again on a separate line.
The takeaway: do not assume what worked at your last job will work here. Re-check every state, every payer.
What to ask your payer before you bill#
Before you submit a claim for collaboration, get five answers in writing from the payer. A short email exchange with the provider relations rep is enough.
- Do you cover care coordination or care collaboration as a separate billable service for ABA?
- If yes, which CPT code do you accept? (Codes that sometimes apply include the 99366 to 99368 family for team conferences and 99451 to 99452 for interprofessional consults. Your payer may use a different code or an HCPCS modifier.)
- What is the monthly or annual cap?
- Does the other professional need to be on the call live, or can it be asynchronous?
- What documentation do you require for a clean claim?
Write down the answer for each client in your billing notes. When a denial comes in three months later, you want a paper trail. And if the payer says no, you have your answer in one round of email instead of three denied claims.
If your clinic has a biller or RCM team, hand them this list. They are usually faster at getting answers than the clinical side.
What to do when collaboration is not billable#
When the payer says no, the worst move is to stop collaborating. Matt was direct about this:
While it's not billable, I still highly highly recommend it.
There are three practical paths when the time is unpaid:
Build it into your existing authorization. Some BCBAs cover collab time during their indirect or protocol modification hours that are already authorized. Talk to your billing lead before doing this, because the rules for what counts as protocol modification vary by payer.
Use it as a clinical lever for outcomes. If a 20 minute call with an SLP cuts two months off a language goal, that is real progress for the client and a real story for your next reauth packet. Outcomes data is the strongest case for keeping a client on service and for justifying the level of care.
Treat it as a business investment. Pediatricians, SLPs, OTs, and school teams refer. A BCBA who shows up prepared, listens, and sends a clean follow up note becomes the BCBA those professionals trust with their next family. That is referral generation, paid for with collab time instead of ad spend.
The hidden ROI: retention, referrals, and discharge timing#
Here is the line from the talk that reframes the math on unpaid collab:
Better outcomes for clients pay off in spades even if these appointments are non-billable.
What does "pay off in spades" actually look like on a P and L? Three places:
Retention. Families stay in care longer when their providers are aligned. Instead of a family pulling their child after six months because nobody is on the same page, you keep them through 18 months and a planned graduation. That is a real revenue swing per client and a much cleaner clinical story.
Referrals. A pediatrician who has had two good calls with you is going to mention your name to the next family who walks in asking about ABA. Matt's framing: that referral is worth more than the 30 minutes you spent on the call, every time. Five to eight strong referrals a year from a single partnership is a realistic number when the relationship is real.
Discharge timing. Collab catches the moments when a client is ready to step down before the BCBA sees it solo. That protects the family from over-service and protects your clinic from a reauth fight when the payer notices the same goals on the plan for two years.
None of this shows up on a billing report. All of it shows up in the next quarter's numbers.
How to track collab time even when you cannot bill it#
If you want to make the ROI case to your clinic owner, you need data. Track collab the same way you would track a billable service. Five fields are enough:
- Date and length of the call
- Who you spoke with (role and discipline)
- Client (de-identified if needed for internal review)
- One sentence on the clinical purpose
- One sentence on the outcome or next step
A Google Sheet works. Your EHR's session note system works. The point is to be able to pull a report at the end of the quarter that shows "BCBA spent 14 hours on collab, attached to 9 clients, with these documented outcomes."
That is what you put in front of an owner who is asking why the schedule has unbilled time on it.
Talking to your clinic owner about non-billable collab#
Owners are not the enemy here. Owners are running a P and L with razor margins. If you walk into the office and say "I need two hours a week for unpaid collab," the owner hears cost. If you walk in with a one page summary that ties collab hours to retention months, referral counts, and reauth wins, the owner hears investment.
Matt has been on both sides of this conversation, as a lead BCBA pitching to founders and as a clinic director hearing pitches. His pattern is the same one he uses with payers: lead with outcomes, back it with numbers, ask for a defined window. "Give me one quarter to track collab against retention on these five clients" is a much easier yes than "I want collab time forever."
Bring the data when it is time to renew the ask.
FAQ#
Is there a CPT code for care collaboration in ABA? There are CPT codes that some payers accept for care collaboration (the 99366 to 99368 team conference family and the 99451 to 99452 interprofessional consult codes are the ones that come up most often), but whether those codes pay out for a BCBA depends entirely on your state and your payer contract. Always confirm with the payer before billing.
Why can I bill for collab in one state but not another? State Medicaid programs write their own ABA rules and commercial payers tend to follow the state lead. Virginia Medicaid recognized care collab time for the plan Matt billed under. Florida Medicaid currently does not. The science is the same; the payer policy is different.
Should I still do collab if I cannot bill for it? Yes. Client outcomes improve, families stay in care longer, and referring providers send you their next family. Those returns are real even when no CPT code applies. The trick is to track the time so you can prove the return.
How do I prove the ROI of unpaid collaboration time? Track every collab touchpoint with date, length, who you met with, clinical purpose, and outcome. At the end of each quarter, pull a report that ties collab hours to retention months, referrals received, and reauth approvals. That packet wins the conversation with owners and billing leads.
Can I bundle collab into another billable session? Sometimes. Some payers let BCBAs cover collab discussion during authorized protocol modification time. The rules vary, so confirm with your biller before assuming this is allowed. Bundling collab into a direct treatment code without payer approval is a fast way to draw an audit.
Keep going#
You now have a framework for the money question. The next step is to build the rest of your collab system: how to stay inside scope, how to handle conflict, how to prep families for the appointments you cannot attend, and how to share the right information without crossing privacy lines.
Watch the full CEU for the clinical and business side together, then explore the related guides below.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Stronger Together: Care Collab with Matt Harrington and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.