Resolving Conflict Between a BCBA and an SLP Without Burning the Bridge
Disagreements with an SLP do not have to end the relationship. Learn how to de-escalate, document, and protect the kid, from a BCBA-led CEU.
Key takeaway
This is the repair manual for the moment when a BCBA and an SLP land on opposite sides of a kid's plan and the working relationship starts to crack. You are not looking for a winner.
Stronger Together: Care Collab
On this page · 9 sections▾
This is the repair manual for the moment when a BCBA and an SLP land on opposite sides of a kid's plan and the working relationship starts to crack. You are not looking for a winner. You are looking for a way back to the table so the kid keeps getting good care. The steps below come straight from a BCBA-led CEU on care collaboration, and they work whether the blowup happened in an IEP meeting, a clinic hallway, or a long email chain that got too sharp too fast.
Why BCBA-SLP conflict is normal, not failure#
If you have been in this field for more than a year, you have probably had a session where an SLP told you that ABA does not work, or an IEP meeting where the speech goals and the behavior plan pulled in opposite directions. That feeling of "we are not on the same team" is not a sign that you failed. It is the default setting of any room where two clinicians care a lot about the same kid and were trained in different languages.
"There will be conflicts. It's not your fault. It is the name of the game."
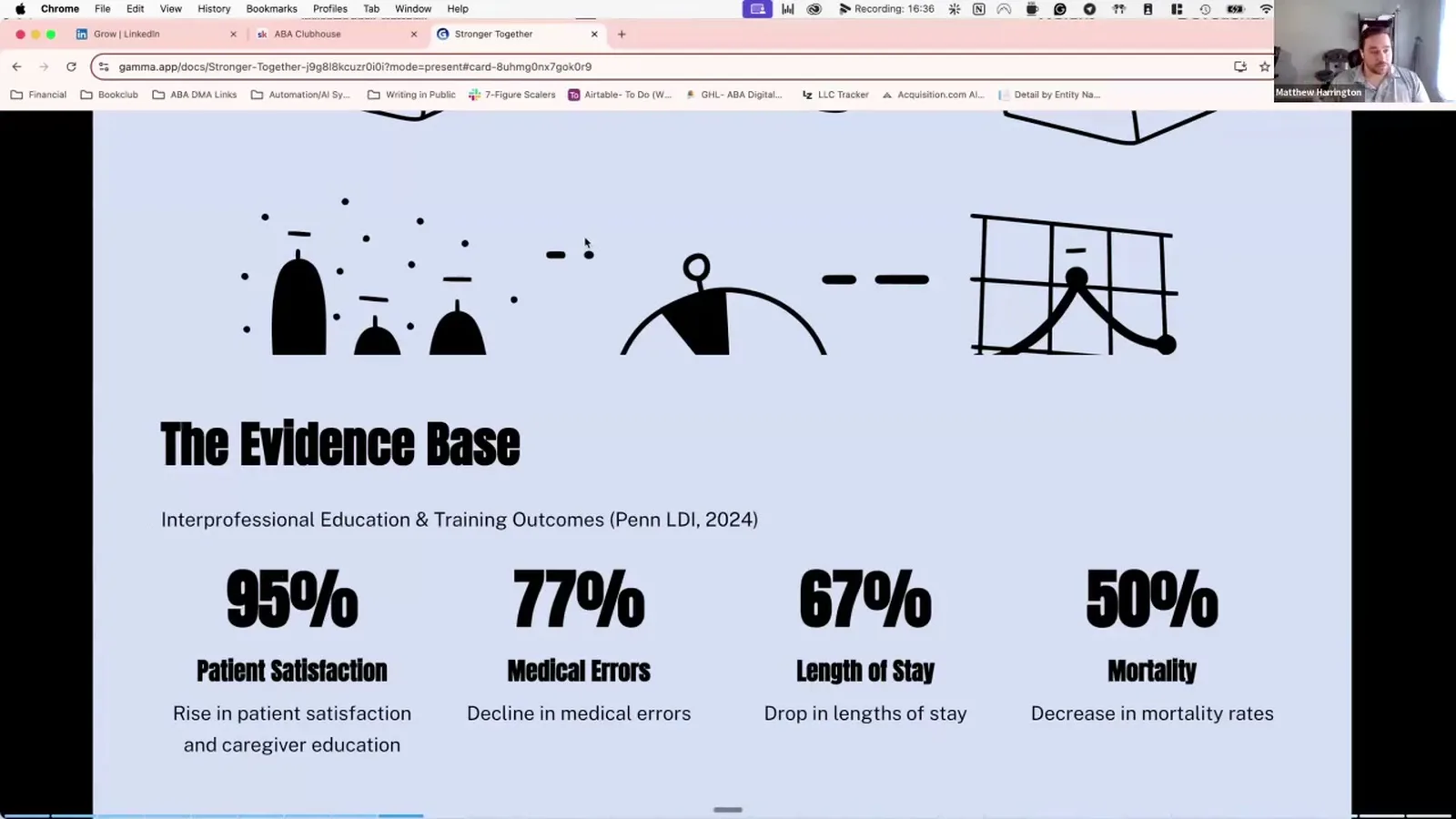
Even hospitals with formal grand rounds had to make care collaboration mandatory because the people inside resisted it. Doctors and nurses, who have worked side by side for decades, still fight about who calls the shots. So when you and an SLP disagree on whether to teach a mand before a tact, or whether to work on AAC before vocal speech, you are running into the same human pattern. Normalize it. The goal is not zero conflict. The goal is conflict that ends with a better plan for the kid.
The credentials measuring contest and how to step out of it#
Most BCBA-SLP fights start the same way. One person says something that sounds like, "Well, in our field we know," or "The research is pretty clear that." It feels harmless from the inside. From the outside, it sounds like a flex.
"Anything that tries to give you an inch higher on them, they interpret that as you're trying to shove them into the ground."
Once the other person feels shoved down, they jump back up. They cite their own research. You cite yours. Now you are in a contest of whose letters after their name are longer, and the kid is nowhere in that conversation. The way out is not to win the contest faster. The way out is to refuse to play. Drop the appeals to "our science says." Ask what they are seeing. Ask what they have already tried. Ask what they would do if they were running your session next week. You are still the BCBA. You still have data. You just stopped using your credentials as a hammer.
Catching the precursors before the IEP blowup#
You already know how to think about precursor behavior with a kid. The same model works on adult conflict. By the time you and the SLP are arguing in front of the parent at an IEP table, you missed about four earlier moments where you could have softened the disagreement in a private email or a five-minute hallway chat.
"You'd want to intervene way early on, even before the precursors."
Watch for the small signs. Slower email replies. Goals that quietly drift in different directions. A parent who starts saying, "Well, the SLP told me." A note in the speech report that subtweets your behavior plan. None of those are emergencies on their own. Together, they are the precursor stack. The earlier you reach out and say, "I want to make sure we are still rowing in the same direction," the smaller the eventual fix has to be. Waiting until the IEP meeting is like waiting until the kid is already in full crisis to introduce a coping skill. It is too late to teach it then.
Deflecting language that lowers the temperature#
When a hard conversation has to happen, the words you pick in the first two sentences set the ceiling for how well it goes. The CEU calls this deflecting language, and it is the single most useful tool in this whole playbook.
"Lots of deflecting language, lots of humbleness. 'I could be totally misunderstanding this.'"
Try openers like, "I could be reading this wrong, but," or "Help me understand how you are thinking about this," or "I am a little confused on the language piece, can you walk me through it?" These phrases do two things at once. They put you in the learner seat, which lowers the other person's guard. And they leave space for you to be wrong, which means if new information shows up, you can update without losing face. You are not being weak. You are being a clinician who knows that the fastest way to a good plan is a calm room.
Using data without weaponizing it#
Data is supposed to help you and the SLP make a better decision together. The trap is using it to prove a point. The second the other person feels like your graph is a "gotcha," they stop reading it.
A better move is to bring the data and then ask a real question. Show the sleep correlation, the rate of mands, the latency to response, whatever you have. Then say, "I am not sure what this means yet. What do you see?" You still get the benefit of being the BCBA who runs the numbers. You also give the SLP a place to add their lens before you lock in a conclusion. The goal is not to be the smartest person at the table. The goal is to get to the best plan with the fewest detours. Sometimes the SLP will look at your data and notice a pattern you missed because you do not live in the speech world. That is a win, not a loss.
Documenting the disagreement for next year#
Even when a conflict ends well, write it down. Not as ammunition. As a gift to next year's version of you, who will probably be at the same IEP table with the same SLP.
Note what each of you proposed. Note what you agreed to try first. Note the data you both said you would collect to know if it was working. Note the date you agreed to revisit it. Keep it factual and short. If the disagreement was real, the documentation lets you skip the warm-up round next time and start where you left off. If the SLP rotates out and a new one comes in, you have a clean record to hand over that is not coloured by your frustration in the moment.
What to do when the other provider truly will not collaborate#
Sometimes you do everything right and the other clinician still will not engage. They miss meetings. They refuse to share their plan. They go quiet for months. At that point, your job changes. You stop trying to win the relationship and start protecting the kid.
Loop the parent in early. Send them your data and your goals in plain language so they can carry it into the next speech session themselves. Document every attempt you made to collaborate, with dates. Stay inside your scope of practice. If the kid needs a swallow study or a formal language assessment, refer out and put that referral in writing. You are not giving up on care collaboration. You are making sure that one unresponsive provider does not become the reason the kid stalls.
FAQ#
Why do BCBAs and SLPs disagree so often?
Different training, different vocabulary, and a long history of each field thinking it should drive the language goals. Most disagreements are not about evidence. They are about who feels respected in the room.
What do I say when an SLP tells me ABA does not work?
Do not defend the field. Ask what experience shaped that view. Most of the time the SLP is reacting to a specific bad BCBA they worked with three years ago. Acknowledge that experience, then bring the conversation back to this kid and what you are both seeing.
Should I escalate to the clinic director or the parent first?
Almost always the parent, with the SLP looped in. The parent owns consent and they can ask both of you to sit down together. Escalating to a director first feels safer but reads as going around the other clinician, which makes the next conversation worse.
How do I document a clinical disagreement ethically?
Stick to facts. What was proposed, what the data showed, what was agreed to, and when you will revisit it. Skip opinions about the other person. Save the documentation where the next BCBA on the case can find it.
What if the other provider just stops responding?
Document your outreach attempts, keep the parent informed, stay inside your scope, and refer out for anything you cannot ethically handle alone. Then keep the door open. Providers come back to the table when they see you are still focused on the kid instead of the fight.
Keep the kid at the center#
Every step in this playbook points back to one rule. The fight is not the point. The kid is the point. When you catch the precursors early, use soft language, share data without weaponizing it, and document the disagreement so future you has a head start, the relationship survives even hard conversations. That is what care collaboration looks like in real life, not in the slide deck.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Stronger Together: Care Collab with Matt Harrington and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.