Trauma-Informed PFA and SBT: What the Enhanced Choice Model Changed
What the Enhanced Choice Model is, what it strips out of classic SBT, and how to run trauma-informed PFA without losing control, from a BCBA-led CEU.
Key takeaway
The Enhanced Choice Model (ECM), described by Rajaraman and colleagues in 2021, is the operational rewrite of Practical Functional Assessment (PFA) and Skill-Based Treatment (SBT) that strips out every piece of physical management, builds in a way to leave at any time, and leans on safety signals and role play instead.
12 days of PFA & SBT
On this page · 9 sections▾
The Enhanced Choice Model (ECM), described by Rajaraman and colleagues in 2021, is the operational rewrite of Practical Functional Assessment (PFA) and Skill-Based Treatment (SBT) that strips out every piece of physical management, builds in a way to leave at any time, and leans on safety signals and role play instead. It is paired with a quiet but bigger shift from Greg Hanley, who started saying we should stop calling it trauma-informed and start calling it trauma-assumed, because we should assume every client has some trauma history rather than wait to be told. The first time most clinicians hear ECM described, the very first question that comes back is not clinical. It is a billing question: if the kid can walk out, can I still bill the session? This page answers both halves. What the model actually changes on the floor, and what to say when your clinical director asks about the insurance code.
What the Enhanced Choice Model Actually Strips Out (Rajaraman 2021)#
Classic SBT, the way Hanley and team built it out across the 2010s, leans on a few things that the Enhanced Choice Model takes off the table. Physical prompts during tolerance training. Blocked escape from the room. A clinician-controlled start and stop to each practice trial. Rajaraman and colleagues in 2021 looked at all of that and asked a simple question: can you run PFA and SBT and still get differentiation without any of it? Their answer was yes, and the procedure they published is the cleanest summary of what the model removes.
Key changes to the PFA and SBT methods include all physical prompting being removed an increase in role play and demonstration that's a reliance on safety signals an increase in choice availability at all times and the opportunity to end the practice session or terminate the session. From the talk — Matt Harrington
That is the whole punchline in one sentence. No physical prompting, more modeling, safety signals (a clear visual or vocal cue that says the hard part is coming or the hard part is over), choice available at every moment, and a real exit door labeled in advance. The thing to notice is what is not in the list. The functional analysis is still there. The synthesized contingencies are still there. The Functional Communication Response (FCR) is still there. The shaping ladder is still there. ECM is not a different treatment. It is the same treatment with the parts that look like restraint pulled out.
Trauma-Informed vs Trauma-Assumed: Why Hanley Switched the Word#
The other half of the shift is a word choice. For a few years the field talked about trauma-informed care, which usually meant "if a client has a known trauma history, we adjust." Hanley walked that back. The new framing is trauma-assumed, and it is not a small change.
Instead of trauma-informed we should really be thinking about trauma assumed care and that's the concept of just assuming that all the people that we serve all the population that we work with probably has some trauma that has been placed on them so they're always going to react very specifically to certain stimuli From the talk — Matt Harrington
Why does the word matter? Because trauma-informed asks the clinician to find the trauma first, then adjust. Trauma-assumed asks the clinician to adjust by default, because most of the families on a BCBA's caseload will never disclose a full trauma history, and many will not know one to disclose. If you wait for permission to strip out physical prompts, you will be too late for half your cases. If you assume the history is there and you build the procedure that way, you are right more often than you are wrong, and you are safer in the cases where you turn out to be right.
Procedures to Audit on Your Current BIP#
This is the part of the talk most clinicians want to write down. If you are sitting with a current behavior intervention plan (BIP) and asking which lines need a second look under a trauma-assumed lens, here is the short list to walk through.
Imagine if you had a child who experienced physical abuse programming a lot of heavy-handed physical prompting even if it was for skill acquisition and not for behavior reduction is probably not a good choice because of their trauma history any amount of physical management it's likely going to re-trigger some of that trauma From the talk — Matt Harrington
Three procedure families are the usual targets:
- Physical prompting and physical management. Even for skill acquisition. A child with any physical-abuse history is going to read a hand-over-hand prompt the same way they read the original event, at least in the body. If you can teach the skill with a model or a gesture, do that.
- Timeout and seclusion-style procedures. A child who has experienced being shut in a room is not going to learn the contingency the way the BIP expects. They are going to learn the room.
- Attention extinction. A child who has experienced abandonment is going to read a planned ignore very differently than your textbook says. The clinical effect may still happen on the data, but the side effects are real.
You do not have to throw the BIP out. You have to know which lines to swap and what to swap them for.
What Replaces Physical Guidance: Vocal and Gestural Re-Prompts#
The single biggest worry clinicians have about ECM is the same one supervisors have: if I cannot physically guide, what do I do when the child is mid-escalation and the FCR is not coming out? Rajaraman and colleagues' answer is the cleanest piece of the protocol.
Positive reinforcers are still withheld during the EO. The escape extinction component is still there in name. What changes is the prompt topography. Instead of a hand-over-hand physical prompt to the FCR card or the FCR vocal, the clinician delivers a repeated vocal prompt and a gestural prompt. The child still has to emit the FCR to get the reinforcer. The clinician is just not their hands anymore. The data the team published shows the FCR still emerges. It just emerges through more modeling reps, not more guidance.
This is the line your supervisor will want a reference for. Rajaraman, Hanley, Strand, Staubitz, and Brewer, 2021, in the Journal of Applied Behavior Analysis.
The "Hang Out" and "Visit Terminated" Conditions, Explained#
ECM gives the learner two structured ways out of the work, and both are part of the program, not a treatment failure.
The first is sometimes called the "hang out" condition. The learner can choose at any moment to step out of the practice trial and into a low-demand area in the same room. The reinforcers from the synthesized condition are still available. The hard part is just paused. The clinician is not chasing. The data are still being taken.
The second is "visit terminated." The learner can choose to end the session and leave. The clinician marks it, the session ends, and the team regroups. The first time a team runs this, the room gets quiet because nobody believes the kid will actually use the option. Most kids try it once, then come back, then stop testing it. The exit door being real is what makes the rest of the procedure work.
Can You Still Bill for a Session a Learner Chose to Leave?#
This is the question that comes up every time, and pretending it does not exist is the fastest way to lose the room.
Oh my gosh like what will we do if insurance uh knows that we let the kid leave like can we not bill and yes super valid concerns and concerns that um I've had when you know promoting this to other people in my company that I work with as well. From the talk — Matt Harrington
The honest answer has two parts. First, billing in ABA pays for the clinician's time, the assessment work, the data, and the treatment delivery, not for a minimum-minute door-locked block. A session that ends because the learner used a programmed choice is still a session with assessment, data, a written treatment note, and a clinical decision attached. Second, the documentation needs to do the work the procedure used to do. The note should say the learner accessed the programmed choice to terminate, the data point that triggered it, and the next-session plan. That is what a clean paper trail looks like, and that is what survives a chart review.
If your funder has a specific minute-floor rule, talk to billing before you launch ECM, not after. This is the conversation most clinical directors are willing to have once they see the data and the literature.
How to Train Your Team Into Trauma-Assumed Practice Without Throwing Out SBT#
The mistake teams make is treating ECM like a brand-new treatment that replaces SBT. It does not. The synthesized contingency analysis, the FCR shaping ladder, the tolerance training, the change-in-criterion design, all of it stays. What changes is a handful of operational defaults: prompt topography, exit availability, safety signals up front, and the trauma-assumed lens applied to every BIP line.
A reasonable rollout is three steps. One, run a team meeting on the four operational changes in the Rajaraman 2021 procedure and walk through one current case file together. Two, pilot ECM on a single client whose family has consented and whose BCBA is comfortable. Three, write the documentation template for "visit terminated" and "hang out" notes before you need them, so billing is not improvising at the end of the week.
Frequently asked questions#
Is the Enhanced Choice Model the same thing as assent-based practice?
They overlap a lot, but they are not the same. Assent-based practice is the broader principle that the learner's ongoing agreement matters and is observable. ECM is one specific procedure that builds assent into PFA and SBT through choice, safety signals, and a real exit. You can run assent-based practice without ECM. You cannot really run ECM without an assent-based mindset.
Do I have to drop all extinction procedures to be trauma-assumed?
No. ECM still uses extinction. The reinforcer is still withheld during the EO. What gets dropped is the physical-management piece of escape extinction. The contingency is still there. The clinician's hands are not the way it gets delivered.
What do I tell parents who think "letting him leave" is reinforcing the problem behavior?
Two things. First, the choice to leave is programmed and is offered before any problem behavior starts, not after, so it is not on a behavior contingency. Second, in the published data, kids who use the exit early stop using it as the FCR comes in. The exit being real is what makes the FCR worth using.
Keep going#
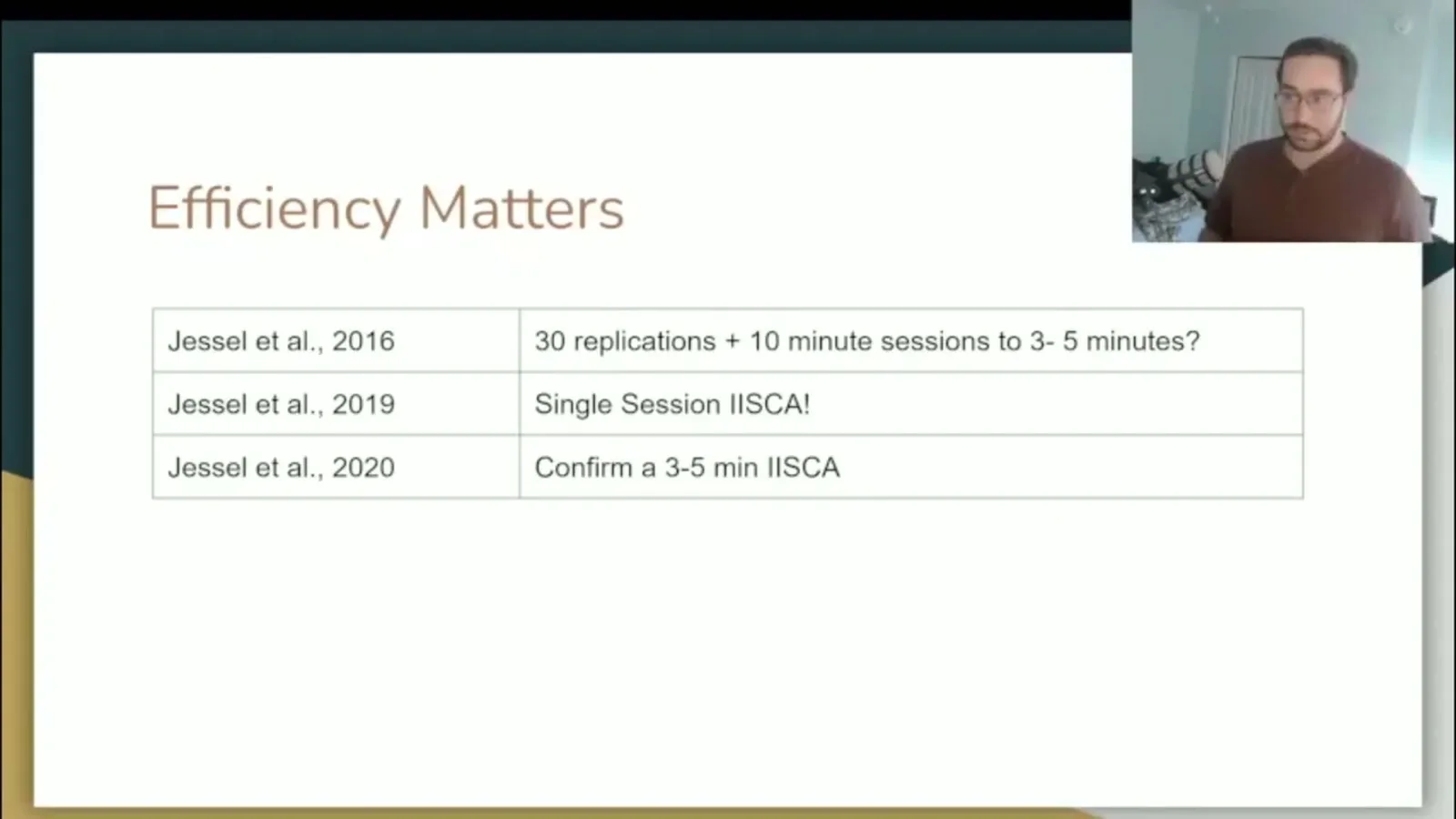
ECM lives inside the larger PFA and SBT framework, and a lot of the operational decisions get easier once the parts around it are clear. The siblings below walk through what PFA and SBT actually are, how synthesized contingencies work, when the single-session IISCA is the right call, and how to shape the FCR from "my way" to a full polite request.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch 12 days of PFA & SBT with Matt Harrington and earn 3 free BCBA CEUs. Detailed certificate, delivered the moment you finish.