Ostrom's 8 Core Design Principles for ABA Teams
Eleanor Ostrom's 8 design principles, translated for ABA clinics. Shared identity, fair decisions, polycentric governance, from a BCBA-led CEU.
Key takeaway
Ostrom's 8 core design principles sort into 3 buckets (coordinate the group, suppress selfish moves, manage between-group relations), and the two principles most ABA clinics botch are CDP 7 (self-governing authority) and CDP 8 (polycentric governance with the bigger world of payers, families, and the field).
On this page · 7 sections▾
Ostrom's 8 Core Design Principles for ABA Teams
Ostrom's 8 core design principles sort into 3 buckets (coordinate the group, suppress selfish moves, manage between-group relations), and the two principles most ABA clinics botch are CDP 7 (self-governing authority) and CDP 8 (polycentric governance with the bigger world of payers, families, and the field). That is the short version. The longer version is that a Nobel-winning economist watched fishers, farmers, and shepherds run shared resources for decades, wrote down what worked, and gave us a checklist that fits a BCBA's team meeting better than most supervision books on the market.
Who Eleanor Ostrom Was and Why a Nobel Economist Matters to BCBAs#
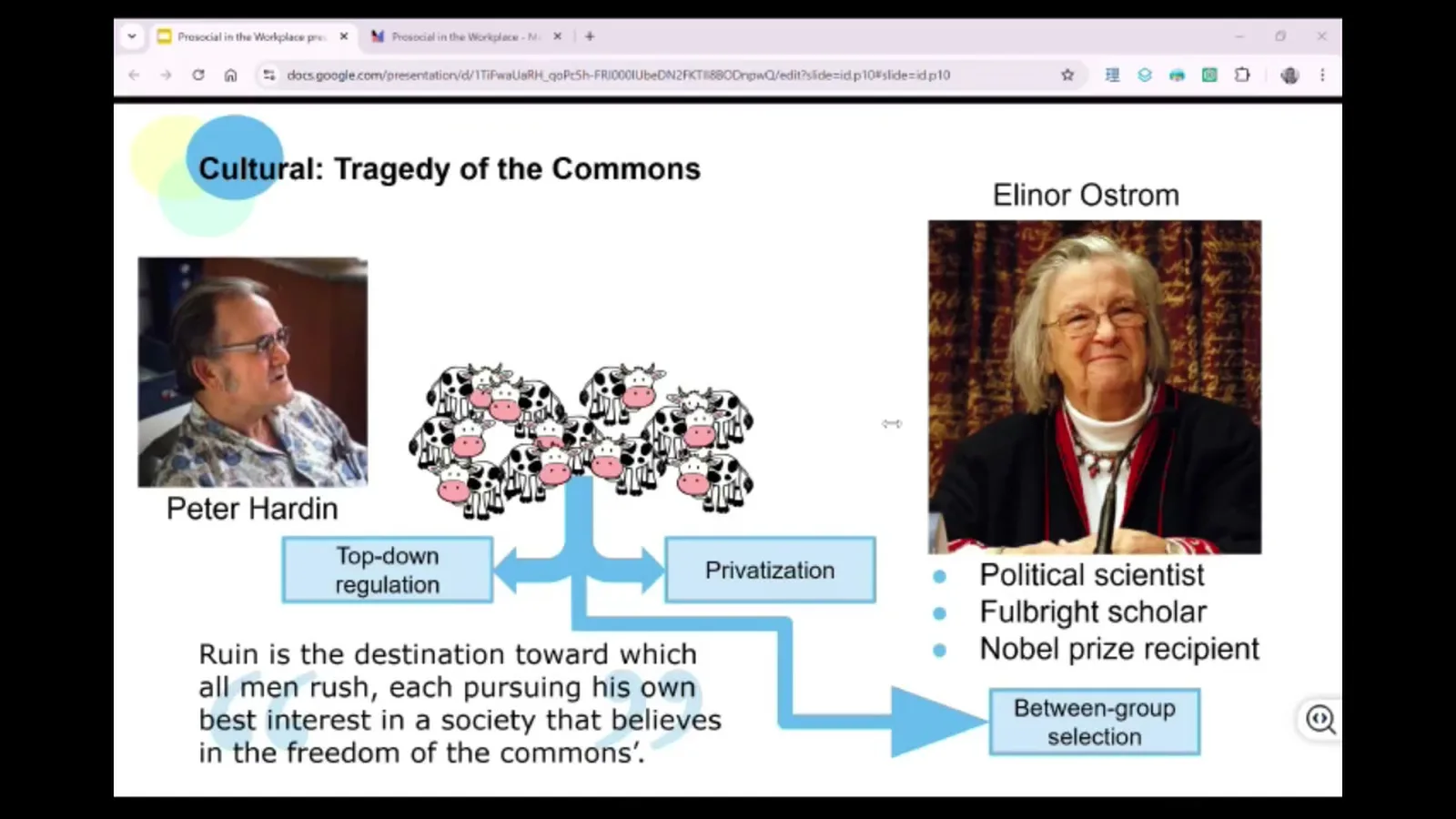
Eleanor Ostrom was a political scientist with a Fulbright. She did field work all over the world watching how groups manage shared stuff, like water, fish, pasture, and forests. In 2009 she won the Nobel Prize in economics for that work. As Jason Stauffer put it in the CEU:
Eleanor Ostrom was a political scientist and Fulbright scholar. She conducted field work across the globe studying group management of common resources. In 2009 she received the Nobel Prize in economics for her work.
Why should a BCBA care? Because your clinic is a common pool. Caseload hours, supervision time, RBT energy, parent trust, payer goodwill. Everyone draws from the same pond. If a few people pump too fast, the pond goes salty for everyone. That is the tragedy of the commons, dressed up in scrubs.
Ostrom did not buy that the only fix is a boss yelling from the top or a private equity firm buying the pond. She found that real groups, on the ground, figured out how to share. Then she wrote down the patterns. Those patterns are the 8 CDPs.
The 8 CDPs, One ABA Example Each#
Here are the eight, each with a quick ABA picture.
- Shared identity and values. Your team can say in one sentence who they are, who they serve, and why. Example: a clinic where every staff member can finish "we exist to..." the same way.
- Fair share of costs and benefits. What you put in lines up with what you get out. Example: the BT who covers Saturday clinics is not the same one who gets stuck with every late note.
- Fair and inclusive decisions. People affected by a rule help make the rule. Example: shift swap policy is built with the techs, not handed down by ops.
- Monitoring. People can see if the group is doing what it said it would do. Example: open dashboards for IOA, session note timeliness, and parent training minutes.
- Graduated responses. Small slips get a small response. Big or repeat slips step up. Example: a missed note gets a check-in; a third missed note triggers a written plan; nothing starts at "you are fired."
- Fast, fair conflict fixes. When two people clash, there is a known path to sort it out. Example: a one-page "if you have a beef with a coworker" flow that does not start with HR.
- Authority to self-govern. The team can make the calls that affect the team without asking permission for every move. Example: the clinical pod picks its own meeting rhythm and case review format.
- Polycentric governance. Your team links up with other groups (other pods, the field, payers) and the same principles run between those groups too. Example: a clinic that co-writes guidance with families and payers instead of just receiving rules from them.
Three Buckets: Coordinate, Suppress Selfishness, Manage Between-Group Relations#
Eight is a lot to hold in your head. Ostrom and the Prosocial team sort them into three jobs.
Bucket one, coordinate the group. CDPs 1 and 3. Shared identity tells the group who it is. Inclusive decisions tell the group how it decides. Without these, the rest is noise. A clinic that cannot answer "who are we for" cannot fairly decide anything else.
Bucket two, suppress the selfish pull. CDPs 2, 4, 5, and 6. Fair share of costs and benefits, monitoring, graduated responses, and fast conflict fixes. This bucket is the one BCBAs already half-know from behavior analysis. We arrange the environment so the short-term selfish move does not pay off more than the team move. As Stauffer put it:
Eight core design principles, or CDPs. They can be grouped into three general categories.
Bucket three, manage between-group relations. CDPs 7 and 8. These are the ones that ask: does your team get to run itself, and does it play well with the other teams it touches? This is where most clinics get stuck, which is the next section.
A note on how to hold these. They are not a checklist of rules to memorize. They describe how a group's environment is set up so that working together pays off. As Stauffer said:
Rather than viewing the CDPs as a checklist of rules, it's more helpful to understand them as describing functional relationships.
For a BCBA that sentence should ring a bell. Functional relationships are our home turf. We arrange antecedents and consequences so the right behavior pays. The CDPs do that at the group level.
CDP 7 and CDP 8 Are Where Most ABA Clinics Break#
CDP 7 is the authority to self-govern. Stauffer framed it like this:
CDP seven... does your group have the authority to make important decisions on its own without outside interference?
In a real ABA company, that question splits into layers. Can the clinic make calls that affect the clinic without waiting on a regional VP? Can the pod inside the clinic pick its own case review format? Can the BT-supervisor pair decide how to run a session debrief? If every layer waits on the layer above, you get learned helplessness, which is what most BCBAs hear from new supervisees: "whatever you think."
CDP 7 is the answer. Push real choices down to the layer that does the work. Not every choice. Just the ones that layer can own. A BT can own how they greet a learner. A pod can own its meeting rhythm. A clinic can own its hiring rubric. When that authority is missing, the people closest to the work stop bringing ideas, because nothing they say sticks.
CDP 8 is polycentric governance. That is a big phrase for a simple idea: your team is one of many, and the same eight principles need to run between teams, not just inside them. For an ABA clinic, the other teams are real and unavoidable: families, school districts, payers, the BACB, RBT training schools, even the private equity group that bought the company last year. CDP 8 asks if your clinic and those other groups share an identity and purpose, share costs and benefits fairly, and have a fair way to settle fights.
This is where ABA gets ugly. A clinic that nails CDP 1 through 6 inside the building can still burn out, because the payer treats it like a vendor, the families feel left out of plans, and the field pulls in five directions. CDP 8 says: you cannot fix that by working harder inside. You have to build the same kind of group out at the level above.
CDP 7 and CDP 8 are also where the cultural and the evolutionary parts of Prosocial meet. Inside the clinic, push power down. Outside the clinic, build shared purpose with the bigger groups you touch. Skip either side and the team falls back into the selfish-pull pattern Ostrom watched ruin fisheries and pastures.
Using the CDP Web Chart to Score Your Own Team#
The Prosocial project built a simple tool for this: a web chart with eight spokes, one per CDP. You can score each spoke two ways.
First, how important is this CDP for our team right now? Second, how well are we doing on it? Use a 0 to 10 scale, or a 1 to 5. Score closer to the center means weaker. Score closer to the outer ring means stronger. You end up with a shape. The shape tells you where to start.
A practical way to run it: pick the group from the talk (your pod, your clinic, your family, your supervision dyad). Score the eight spokes solo first. Then have each person on the team score, and lay the shapes on top of each other. The gaps between scores are usually more useful than the average. If you rate CDP 3 (fair decisions) a 9 and your BT rates it a 2, that gap is the conversation.
Pick one low spoke and one small move. CDP 1 low? Run a 15-minute "who are we, who do we serve, why" session. CDP 7 low? Hand one real choice to the pod this week. CDP 8 low? Set up one shared meeting with a referring SLP, school, or family advisor. Rescore in a month.
The point of the chart is not to grade your team. It is to give you a clean, behavior-friendly target. As BCBAs we are good at picking one target behavior at a time. The CDP chart turns team culture into the same kind of target.
Frequently Asked Questions#
What are the 8 core design principles in simple words? Know who you are, share costs and benefits fairly, decide together, watch what is happening, respond in steps, settle fights fast, run your own group, and play well with the other groups around you.
How do I apply CDP 1 (shared identity) in a busy ABA clinic? Block 15 minutes at your next team meeting. Have everyone finish two sentences: "we exist to..." and "we are the kind of team that..." Compare answers. The gaps are your work.
What does polycentric governance look like for an ABA company? It looks like the same eight principles running between your clinic and the groups around it: families, schools, payers, the wider field. Shared purpose, fair share, fair decisions, real monitoring, all at the bigger level.
How do graduated sanctions work without feeling punitive? Small slips get small, kind responses. Repeat or big slips step up in clear stages. Everyone knows the stages ahead of time, so nothing feels personal or random.
Can I use the CDP web chart with my team next week? Yes. Pick the group, draw eight spokes, score each one solo, then together. Pick the lowest spoke and one small move for the next month.
Take the Full CEU#
This page is a map. The full CEU walks the bigger Prosocial frame around these principles, including how language and psychological flexibility plug in. It is taught by Jason Stauffer, BCBA, and is free.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Prosocial in the Workplace with Jason Stauffer and earn a free BCBA CEU. Detailed certificate, delivered the moment you finish.