Direct vs Indirect Contingency Management: When ACT Belongs in Your Plan
Tom Sabo's decision flow for when direct contingency management is enough and when to add ACT, in plain words, from a BCBA-led CEU.
Key takeaway
Tom Sabo opens the talk with a flowchart that gates the entire decision: before you reach for Acceptance and Commitment Training (ACT), you start, and usually finish, with direct contingency management (DCM), the everyday work of defining a behavior, running an assessment of what keeps it going, building a function-matched plan, and only stepping over to the right side of the chart when the plan stalls.
From Research to Practice: Seven Acceptance and Commitment Training Practices You Can Begin Using Today
On this page · 9 sections▾
Tom Sabo opens the talk with a flowchart that gates the entire decision: before you reach for Acceptance and Commitment Training (ACT), you start, and usually finish, with direct contingency management (DCM), the everyday work of defining a behavior, running an assessment of what keeps it going, building a function-matched plan, and only stepping over to the right side of the chart when the plan stalls. That is Practice 1 of the seven, and Tom names it first on purpose. ACT is the detour. DCM is the road.
What direct contingency management is, in one paragraph#
DCM is the work a Board Certified Behavior Analyst (BCBA) learns in grad school. You pick the behavior. You write a clear definition. You gather indirect data from interviews and rating scales. You gather descriptive data from real sessions. You form a guess about what is keeping the behavior going. If you can, you test that guess with a functional analysis. You build a plan that matches the function. If it works, you program for generalization and maintenance and you move on. The whole loop runs on the real, here-and-now consequences in the room. Reinforcers. Setting events. Antecedents you can touch. Nothing fancy. Nothing new.
What counts as indirect contingency management#
Indirect contingency management is Tom's borrowed term from Dick Malott. It covers the work you do when the thing standing between your client and change is not in the room. It is in their head. It is the rule they keep telling themselves. It is the thought that sticks. It is the feeling they will do almost anything to push away. ACT lives on this side of the chart. So do the assessment tools that pull covert verbal behavior into the open so you can work with it. You are still a behavior analyst. You are still tracking observable behavior. You are just adding a class of tools for the verbal stuff that gets in the way.
Number one, if you're working in applied behavior analysis, identify and use direct contingency management strategies. I'm going to show you a flow chart and I'm going to prepare you before I show it to you. It's going to make your eyes hurt. From the talk — the panel
The one question that decides which side to use#
Here is the gate. You have run your DCM plan. It did not work the way you hoped. Before you reach for ACT, ask one question about the person in front of you: can they relate two things on the basis of cues that have nothing to do with how those things look or feel? Can they take a coin and a bill and treat one as worth more in one moment and the other as worth more in the next, just because someone said so? Can they treat two unrelated objects as the same in one frame and as opposite in another? In the field this is called arbitrarily applicable relational responding. In plain words: can they make stuff up about how things connect and then act on that made-up connection?
If the answer is yes, ACT is on the table. If the answer is no, ACT is not on the table. That is the whole gate.
If the client cannot relate things arbitrarily: what to do#
If the client cannot do this, you do not get to add ACT. You go back to the left side of the chart. Tom is direct about it. The plan did not fail because you needed a fancier tool. The plan failed because you missed something in the assessment. Maybe the descriptive data was thin. Maybe the functional analysis tested the wrong condition. Maybe the maintaining variable shifted when the setting changed and you never caught it. The fix is more DCM, not different DCM. Tighten the assessment. Re-test the function. Rebuild the plan to match.
If the person that you're working with cannot do any of these things, well, then you're back to the left-hand side. You miss something in your descriptive assessment and functional analysis. Fine-tune that to identify the maintaining variables for their unwanted behavior. From the talk — the panel
This is the rule that protects the field. ACT is not a rescue tool for any plan that stalls. It is a tool for a specific kind of problem in a specific kind of learner. If the learner is not there yet, you do not borrow a tool that does not fit. You sharpen the one that does.
If the client can: the ACT path Tom walks#
If the client can relate things arbitrarily, then something verbal is probably in the mix. The client is telling themselves something, often silently, that is gluing their behavior to a rule the room cannot see. Your next job is to assess that covert verbal behavior. You bring it into the open. You ask. You watch. You test whether what the client reports they are saying to themselves lines up with what their behavior shows they are saying. Then you build procedures that loosen the glue. ACT calls one family of these procedures defusion. Another family is values work. Another is present-moment training. Each one is aimed at a specific kind of verbal stickiness.
You do not run ACT instead of the plan. You run ACT to unblock the plan.
Returning to direct contingencies at the end#
This is the part that Tom drives hardest. ACT is not where you end. DCM is where you end. Once the verbal block loosens, you come back to the left side and you make the original DCM plan work in the real context. The behavior contract. The reinforcement schedule. The teaching procedure. The data sheet. All of it. ACT is the side trip you took because the road was blocked. The destination did not change.
If you're successful, at that point, you come back to direct contingency management. You should be able to make the direct contingency management strategies that you had developed work for your context. That's where we begin and end in applied behavior analysis. From the talk — the panel
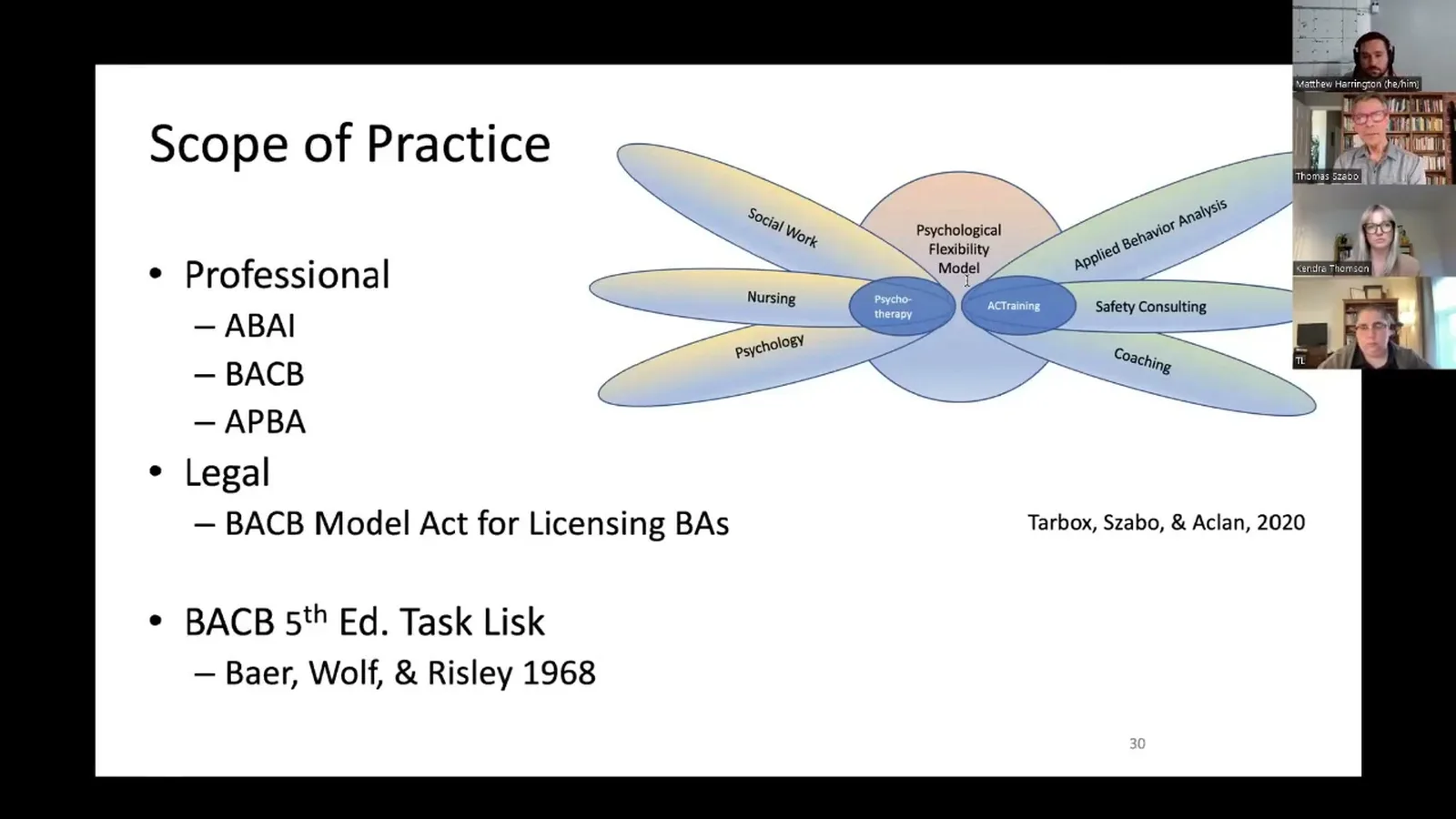
This is also the part that keeps the work inside the BCBA scope of practice. Psychologists can set goals like "be more mindful" or "develop self as context." A BCBA cannot. A BCBA writes goals that map to the fifth edition task list and to observable behavior change. ACT inside ABA is acceptance and commitment training, not therapy, and the training is in service of a behavior goal on a treatment plan that you could defend to a parent, an insurer, or a peer reviewer.
A worked example using the talk's framing#
A nine year old named Juan is having a hard time getting along with his autistic brother Carlos. You define the target. You gather indirect data from the parents. You watch sessions. You form a guess. You build a DCM plan with a level system that pays off shared video game time. You run it. It stalls.
You ask the gating question. Juan is nine. He can take two unrelated things and call them the same, opposite, more, less, depending on what someone said five minutes ago. The gate is open. So you assess the covert stuff. Juan keeps telling himself Carlos "has to" have everything his way. The "has to" is sticky. It is a rule that is fused to his behavior with Carlos. You build a defusion procedure: Juan says the "has to" line in funny voices to loosen its grip. You build a flexibility move: a "ninja walk away" he can use when Carlos's rigidity flares. You teach both. You watch the verbal repertoire shift.
Then you go back to the level system. The DCM plan that stalled now works, because the verbal block is no longer in the way. You program for generalization across rooms and across days. You program for maintenance with a thinning schedule. You take data the whole time. ACT was the detour. The plan was the road.
Frequently asked questions#
How do I assess whether a client relates things arbitrarily?
Watch for it in the natural language sample first. Can the client treat two unlike things as the same when you tell them they are? Can they treat the same two things as opposite when the frame changes? Can they shift which thing is worth more based on a verbal cue? If the client is verbal and old enough, you can probe with simple sorting and comparison tasks. The point is not a formal score. The point is a yes or no on whether arbitrary relating is part of their repertoire. If you cannot get a clean yes from real samples, treat it as a no and go back to DCM.
Is indirect contingency management the same as verbal behavior intervention?
No. Verbal behavior intervention in the classic sense teaches mands, tacts, intraverbals, and other operants. Indirect contingency management, the way the panel uses the term, is the broader category of procedures that work on covert verbal behavior, including the rule-governed stickiness that ACT targets. There is overlap, but they are not the same tool.
Can I run direct contingency management and ACT at the same time?
You can, and most of the time you should. The DCM plan stays running while you add the ACT procedures. The data on the original target behavior keeps coming in. The reinforcement schedule keeps paying off. ACT is layered on to unblock a specific verbal barrier, not bolted on as a separate plan. If you find yourself running two plans that do not talk to each other, something is off. Pull back to the chart.
Where to go next#
If you want to see how this decision rule plays out in the rest of the panel's seven practices, the recording is worth the hour. The next pieces in this series take pieces of the talk and build them out: the defusion exercise where the client phones a sticky thought, the present-moment writing drill, the ACT-extended behavioral contract, and how to write ACT goals on a prior authorization that a payer will actually approve.