Writing ACT Goals on BCBA Prior Auths That Insurance Will Approve
How to write ACT-informed goals on insurance prior authorizations using the BACB task list, with verbatim examples, from a BCBA-led CEU.
Key takeaway
To get an Acceptance and Commitment Training (ACT) goal approved on a Board Certified Behavior Analyst (BCBA) prior authorization, write the goal in the words of the Behavior Analyst Certification Board (BACB) fifth or sixth edition task list, not in ACT vocabulary, and put the ACT piece in the procedures section instead.
From Research to Practice: Seven Acceptance and Commitment Training Practices You Can Begin Using Today
On this page · 9 sections▾
To get an Acceptance and Commitment Training (ACT) goal approved on a Board Certified Behavior Analyst (BCBA) prior authorization, write the goal in the words of the Behavior Analyst Certification Board (BACB) fifth or sixth edition task list, not in ACT vocabulary, and put the ACT piece in the procedures section instead. That is Practice 3 from the panel's seven practices, and it is the single move that decides whether a payer pays for the hour or sends the auth back.
Why insurance reviewers reject ACT-flavored goals#
A payer reviewer is not reading your plan to argue with you. They are reading fifty plans before lunch. Their job is to match every goal to a billable behavior change. If the words on the goal line are not observable behaviors, the auth gets kicked back. It does not matter how good your clinical reasoning is. The form failed the form check.
Tom said this out loud on stage, and it is the reason this page exists.
I've seen prior authorizations get rejected from insurance companies because people have written, my goal is that somebody develops self in terms of context or that they become diffused from their thoughts about the way things are supposed to be. Well, those are cool goals, but they're not applied behavior analysis goals. From the talk — the panel
"Self as context" is not a behavior. "Defused from thoughts" is not a behavior. A reviewer cannot count it, cannot time it, and cannot tell you what changed. So they deny it. That is not a problem with ACT. That is a problem with the goal line.
The rule the panel uses: task list items, not ACT jargon#
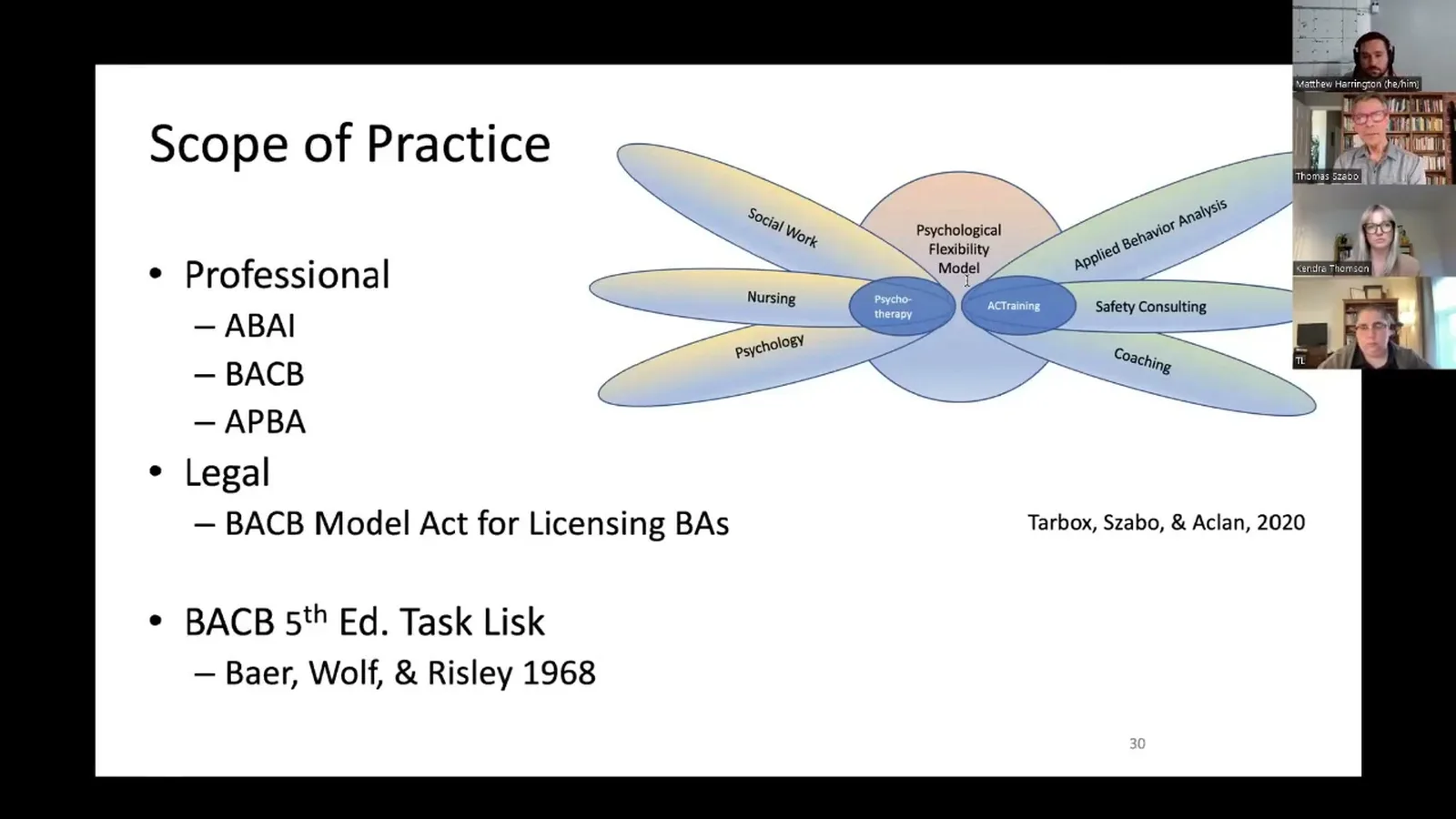
The fix is small and boring. Use the BACB task list as your dictionary. The fifth edition task list, soon the sixth, is the language the payer expects, the language your supervisor expects, and the language the state law on scope of practice was written in. ACT fits inside that dictionary. You just have to translate.
It's a better idea to write your prior authorizations in terms of the fifth edition task list, soon to be the sixth edition task list of the behavior analyst certification board. And fortunately, acceptance commitment training is consistent with the fifth edition task list. From the talk — the panel
So the rule is this. The goal line is written in task list verbs. The procedure section is where the ACT piece lives. The rationale section is where you name the value, the family's words, and the function. Three sections, three jobs. Do not mix them.
The mapping table: 7 task list items to ACT processes#
Here is the panel's mapping, put in the order you will use it when you write the plan. Print this. Tape it to the wall next to your monitor.
- F3, identify and prioritize socially significant behavior change goals. This is the values interview turned into a target list. In ACT terms, committed action. The goal line says what the learner will do more of. The rationale section says why the family picked it.
- G1, use positive and negative reinforcement procedures to strengthen behavior. The reinforcement schedule for the new behavior. In ACT terms, building positive reinforcement into hard tasks. Name the reinforcer. Name the schedule.
- G2, use interventions based on motivating operations and discriminative stimuli. Self-rules that change the value of escape, like "I can be a ninja about this." In ACT terms, conditioned motivating operations that augment distal reinforcers. Document the rule and the moment it gets cued.
- G6, use instructions and rules. Teaching the learner to follow rules when rules help and to drop rules when the setting changes. In ACT terms, working on rule-constricted behavior. This is where flexible responding lives in the plan.
- G10, teach simple and conditional discriminations. Multiple exemplar training across settings, people, and tasks. In ACT terms, sorting situations that look the same but call for different responses. Track the exemplars.
- G19, use contingency contracts. The values matrix or extended behavior contract counts here. Attach the form. Name it.
- G22, use procedures that promote maintenance. The fade plan. The generalization probes. Write the steps for moving from three days a week to four, from a tangible reinforcer to a natural one.
Every ACT piece in your plan should point at one of those seven items. If you cannot point, do not write it.
Content area F3, identify and prioritize socially significant behavior change goals. What does that translate to in ACT? That translates to committed action. G1, use positive and negative reinforcement procedures to strengthen behavior. Well, ideally in ACT, we're primarily focusing on the appetitive. From the talk — the panel
Two before-and-after rewrites of a real auth goal#
Pull a goal from a real auth you have already written. Run it through the rewrite.
Before, version one. "The learner will increase psychological flexibility around demands from his younger brother."
This is a flag. "Psychological flexibility" is a class, not a behavior. There is no count. There is no setting. A new staff member could not score it. A reviewer will deny it.
After, version one. "The learner will engage in cooperative video game play with his younger brother for thirty consecutive minutes, on three days per week, after both children complete homework, for four consecutive weeks."
Same kid. Same clinical plan. New words. The G6 piece, learning to drop the "things have to go my way" rule, lives in the procedure section. The G19 contract is attached. The G22 fade plan moves him to four days, then five.
Before, version two. "The learner will become defused from sticky thoughts about peer rejection during recess."
Again, the goal line is a private event. A reviewer cannot score "defused." The auth will come back.
After, version two. "The learner will initiate one play bid with a peer per fifteen-minute recess period, on four of five school days, for three consecutive weeks." Under the procedure section, you document the defusion teaching, like phoning the sticky thought, and you map it to G2 and G10.
The clinical work did not change. The wording did. The plan now ships.
Words to keep out of the goal field#
Make a do-not-use list and tape it next to the mapping table. The panel called these out by name.
- Acceptance
- Defusion
- Self as context
- Psychological flexibility
- Mindfulness
- Willingness
- Present-moment awareness
- Cognitive fusion
- Values clarification
Each one is a class label, not a behavior. Each one belongs in your training notes, your matrix sheet, and your conversation with the family. None of them belongs on a goal line that a payer will read.
If you really want to keep the ACT vocabulary near the goal, put it in parentheses next to a task list code. Example: "Procedure: phone-the-thought defusion exercise (G2, conditioned motivating operation; G10, conditional discrimination)." The reviewer scans the codes. The codes pass. You keep the ACT teaching intact.
How to document the ACT piece in the procedures section instead#
The procedures section is the right home for ACT. A reviewer expects to see teaching steps there. Write them the same way you would write a discrete trial program.
For each ACT teaching move, write:
- What it is. One sentence. "Practice phoning a sticky thought during a five-minute warm-up."
- When it is cued. The antecedent. "Before any task the learner has previously refused."
- What the staff does. The prompt. The model. The fade.
- What the learner does that counts. The observable response. "Names the thought out loud and proceeds with the task within thirty seconds."
- What gets reinforced. The schedule. Tie it to G1.
- What task list item it maps to. Write the code in the margin.
That format reads like a behavior plan because it is a behavior plan. The ACT label is invisible to the reviewer. The teaching is intact for your staff.
A one-paragraph script to use if a goal gets denied#
When the denial letter arrives, do not rewrite the whole plan. Most denials are wording denials. Use this script in your appeal, swap in your codes, and ship it back the same day.
"Thank you for the review. The goal in question is a socially significant behavior change goal under BACB fifth edition task list content area F3. The dependent variable is observable and measurable, as required by the seven dimensions of applied behavior analysis. The intervention combines positive reinforcement procedures (G1), motivating operation interventions (G2), and rule-based instructional procedures (G6). Generalization and maintenance steps are documented under G22. We have updated the goal-line wording to reflect the task list framing and removed terminology that may have read as outside scope. Updated language is below. Please reopen the authorization."
Six sentences. Codes a reviewer can recognize. New wording attached. Most denials clear at that point. The ones that do not clear are usually about session count, not goal language.
That is the whole point. Keep the ACT teaching in your plan. Keep the task list on your goal line. Use the panel's rule.
Bottom line, take home, make use of the task list when you are writing prior authorization goals that include an attention to interfering covert behavior, rather than writing about the interfering covert behavior as a goal. These are not our goals. They're merely stops along the way. From the talk — the panel
Frequently asked questions#
Can I use the word "defusion" anywhere in a BCBA prior authorization? Yes, but only in the procedure section, and only next to a task list code. On the goal line, never. The goal line is for observable, measurable behavior. The procedure section is where you describe how you teach. If you write "defusion practice (G2 motivating operation; G10 conditional discrimination)" inside a procedure, the reviewer scans the codes and moves on. If you write "the learner will become defused" on the goal line, the auth comes back.
Does Tricare accept ACT-informed BCBA goals? Tricare accepts BCBA goals written against the task list, just like other payers. The panel did not call out Tricare specifically, and you should always check your regional contractor's most recent ABA guidance. The general pattern holds. Task list framing on the goal line passes. ACT vocabulary on the goal line does not. Keep the ACT teaching in the procedures section and reference the matrix or contract as your G19 documentation.
Should I list the BACB task list code next to the goal on the prior auth? Yes. It costs you nothing and saves the reviewer a step. Put the code in parentheses after the goal or in a "task list crosswalk" column. Some payer forms have a slot for this. If yours does not, add it to the rationale section. When the reviewer is the one connecting "G6 use instructions and rules" to your work on rule-constricted behavior, the auth lingers. When you connect it for them, the auth ships.
Watch the full talk#
The panel walks through all seven practices in the recording. The prior authorization section runs in the middle and the task list mapping sits on a slide you will want to screenshot. If you write auths for a team, pull the slide and the script into your supervision agenda this week.