How to Apply Research to One Learner When Your Caseload Is Messy
A worked process for adapting a published intervention to one real client when staffing, setting, and skills do not match, from a BCBA-led CEU.
Key takeaway
In one talk, Matt Harrington walks through three real cases where the same N=1 application process held up: shaping SBT into a school setting for a 14 year old after the district changed his placement, stitching six or seven articles together so an 18 year old could work shifts at a coffee shop, and using multiple schedules plus percentile shaping so a 3 year old could sit in a church pew.
Research to practice - extending past the pages
On this page · 10 sections▾
How to Apply Research to One Learner When Your Caseload Is Messy
In one talk, Matt Harrington walks through three real cases where the same N=1 application process held up: shaping SBT into a school setting for a 14 year old after the district changed his placement, stitching six or seven articles together so an 18 year old could work shifts at a coffee shop, and using multiple schedules plus percentile shaping so a 3 year old could sit in a church pew. None of those clients matched the participants in any single paper. The process for getting from PDF to plan is what stayed the same.
Start with the learner profile, not the intervention#
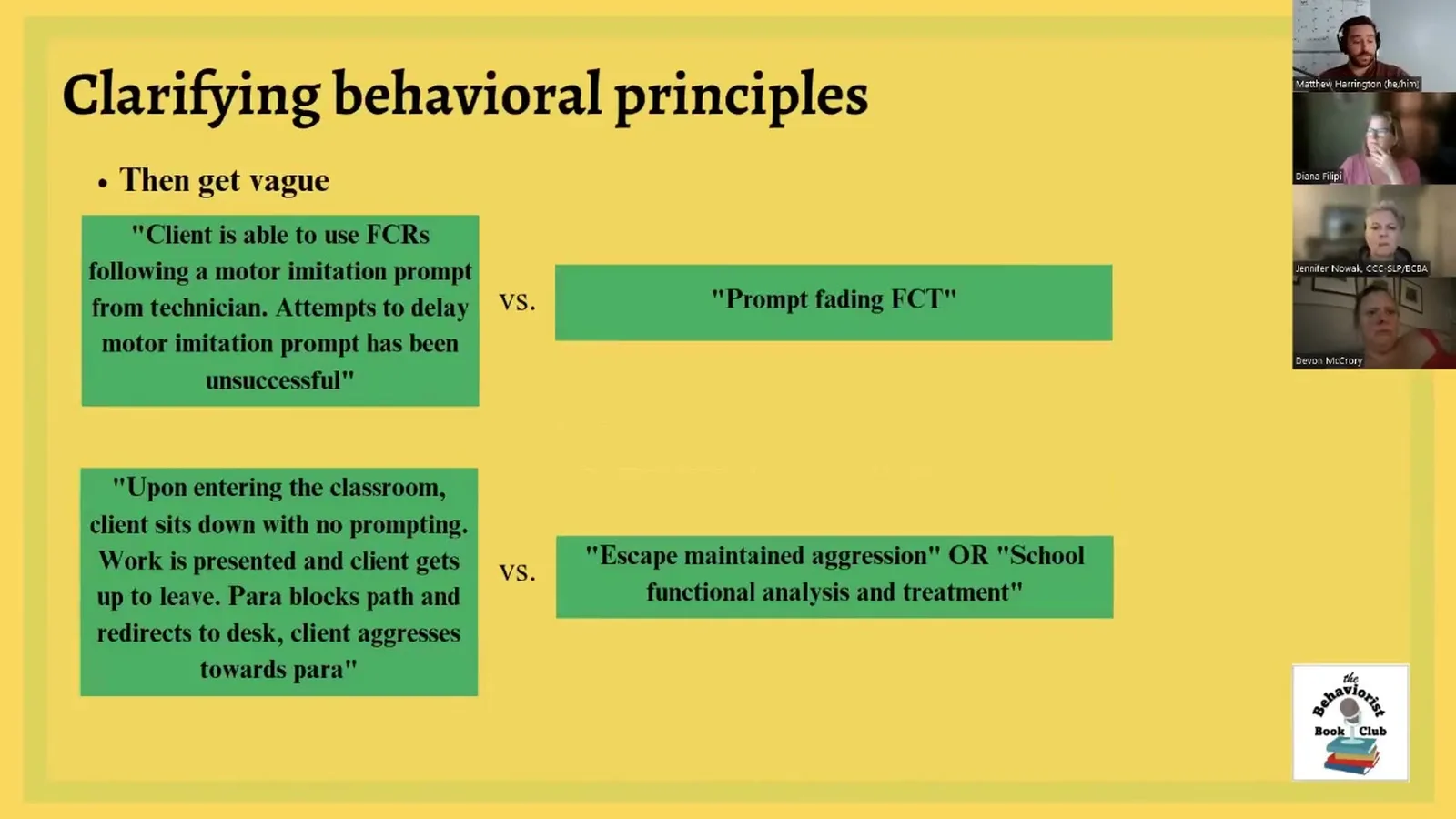
Most BCBAs open Google Scholar before they finish describing the client. That is backwards. The first move is to write out the specifics of the case: what skill is missing, what behavior is showing up instead, what the environment looks like, what motivation is in play, what staff and family can actually do. Get specific before you get vague. Once you can describe the clinical hinge in one sentence, then you back out to the vague version of that sentence and use it as the search term. "Client is not progressing in FCT" becomes "we cannot delay the motor imitation prompt," which becomes the search "prompting AND fading AND functional communication training."
The point of starting with the learner is that you will be ruling research in or out based on whether the behavioral principle in the paper matches the principle in your case. If you do not know the principle in your case, you cannot judge the paper.
Find the active ingredient that maps to your client's barrier#
A research article is doing one thing well. Pull the principle out of the wrapping. The tooth brushing example from the talk is the cleanest version of this. A BCBA asked for a paper on tooth brushing. There is a strong shaping paper on tolerating dentist visits. The dentist paper is not about tooth brushing on the surface, but the active ingredient is shaping tolerance for an aversive head and mouth routine. That is the same active ingredient you need.
When you read a paper, write down the principle in one line. Reinforcement schedule thinning. Demand fading. Multiple schedule signaling. Percentile shaping. That one line is what you carry into your client's plan. The topography in the paper is just packaging.
"It wasn't that she didn't know that we needed to use research. It's that she couldn't extrapolate the principles of behavior change, the valuable nuggets from the research, and then apply them to the totally separate situation where the principles are similar enough."
Pulling pieces from multiple articles instead of forcing one fit#
For the 18 year old at the coffee shop, no single paper covered "teach an autistic young adult to work shifts at a Panera." Matt pulled six or seven articles. One gave him the vocational skill list. One framed values work so the cafe became a meaningful context, not a contrived one. One supported the use of contingent reinforcement over non-contingent reinforcement for keeping behavior in place once staff faded. One spoke to renewal mitigation so gains held up when the support changed. Stack the principles, then write the case conceptualization.
This is the part graduate school skips. You are not citing one paper. You are assembling a small reading list, and each paper earns its spot by closing one gap in the plan.
"There is no research article that talks about how to do vocational skills at a coffee shop. But by pulling things together, we start to clearly get an answer."
Pre-running the procedure in your head with your actual staff#
Before the plan goes live, walk it. Out loud, on paper, in a sync with the team. Who is going to deliver the prompt. What does the data sheet look like. Where does the reinforcer come from. What happens if the learner withdraws assent. What happens if the parent is not in the room.
A lot of feeding research and a lot of strong functional analysis work was run by the first author or by PhD level staff with constant supervision. That is not your caseload. If the procedure assumes a level of fidelity your 19 year old technician cannot hit yet, the plan does not work even if the principle is correct. Pre-running the procedure surfaces those mismatches before you spend three weeks on a graph that will not move.
What to do when the setting changes mid-treatment#
The 14 year old client in case study one started in the outpatient clinic, which lined up neatly with the 2014 Hanley paper that inspired the plan. SBT was working. Then the district moved him to a new school placement and the family lost the appeal. The first two mornings in the new school were back to square one.
The reaction is not to scrap the research. It is to ask what changed and whether the changes touch the principle or just the packaging. The principle behind SBT here was building tolerance for unpredictable schedules of reinforcement and unpredictable transitions. Both of those still applied in the new school. The setting changed. The motivating operations did not. So the plan was shaping SBT into the school, step by step, until the learner was walking into all of his classes on his own.
"We still have a solid intervention based on the research paper because the variables that changed weren't significant enough."
When the setting moves on you mid-treatment, write down which variables changed. If those variables are not the active ingredient, you do not need a new paper. You need a new shaping plan with the same intervention.
Tracking your modifications so you can defend them#
Every time you move away from what the paper did, write it down. Not in a journal. In the clinical record. "Paper used five second prompt delay. We used three seconds for sessions one through six and faded to five by session twelve because of staffing." "Paper ran in outpatient clinic. We ran in a Catholic church for sixty minutes with caregiver as implementer."
Two reasons. First, a future supervisor or auditor can see why the plan looks the way it looks. Second, if the plan stalls, your modification log tells you where to look first. You did not just run "SBT." You ran SBT with these specific tweaks, and one of them is probably the lever.
Knowing when the modification has stretched too far#
The rule from the talk: similar, not exact. You can move setting. You can move age within reason. You can swap staff competence by adding training. You can change topography of the target behavior if the function and principle still fit. What you cannot do is keep the title of the paper and quietly change the behavioral principle. That is when you go back to search and pull a different article.
"We need similar, not exact. We don't want vast differences."
A useful self-check: if you had to defend this plan to the paper's first author, could you explain which principle you kept and which surface features you adjusted? If the answer is "I kept the name of the procedure but nothing else," the modification has stretched too far and the literature is not really backing you anymore.
FAQ#
How do I know if my client is similar enough to the participants?
Match on the behavioral principle and the prerequisite skills the intervention assumes, not on age or diagnosis. If the paper relies on a learner who can tolerate a brief delay to a strong reinforcer, your client needs that skill or a shaping plan to build it. Age and diagnosis are tiebreakers, not gatekeepers.
Can I combine procedures from more than one article?
Yes, and for messy cases you usually have to. Pick one paper as the spine of the plan, then add papers that close specific gaps such as motivation, generalization, or maintenance. Write each pull in the case conceptualization so the team can see why every piece is there.
What if my setting is completely different from the study?
Setting is a packaging variable. Ask if the motivating operations, the response requirement, and the reinforcement source can be reproduced in your setting. If yes, run the same principle with a shaping plan tailored to the new environment. If the setting carries the effect (constant nursing supervision, full PPE, one-to-one ratio), then the paper is not portable as written and you need a different one or a heavier modification.
How do I document modifications for clinical records?
List the paper, the principle you pulled from it, and every place your plan deviates from the published procedure with a one-line reason. Keep this with the BIP or treatment plan, not in a separate doc. If outcomes change later, you can see which modification to revisit first.
When should I stop and look for a different article instead?
When the modifications you are making touch the behavioral principle, not just the packaging. If you have changed the schedule of reinforcement, the contingency, or the target response class so much that the original paper would not recognize the procedure, the literature is no longer backing the plan. That is the cue to go back to search.
Where to go next#
The companion talks in this cluster pair well with this one. If your team is still building the upstream skill of pulling principles out of articles, watch the journal article reading guide and the journal club setup pieces first, then come back here for the application step. If you are heading the other direction, into writing this up as a single subject design, the related guides on translating research to a BIP and evaluating research quality will help you close the loop.
Watch the full talk#
The full hour with all three case studies, the graphs, and the live walk through of the search process is on openceu.com. One CEU.
Turn this topic into a CEU
You just studied this. Now get credit for it.
Watch Research to practice - extending past the pages with Matt Harrington and earn 1 free BCBA CEU. Detailed certificate, delivered the moment you finish.