Relationship-Based ABA Therapy: What It Looks Like in Real Sessions
Plain-language explanation of relationship-based ABA, why pairing is not enough, and what to do instead from a BCBA-led CEU.
Key takeaway
Relationship-based ABA therapy is the version of ABA (applied behavior analysis, the field) where the BCBA (board certified behavior analyst, the clinician who runs the case) builds a positive reinforcement paradigm with the kid first, before any instruction starts.
The Heart of ABA Service Delivery: Creating Connected Relationships - Applied 2023
On this page · 9 sections▾
Relationship-based ABA therapy is the version of ABA (applied behavior analysis, the field) where the BCBA (board certified behavior analyst, the clinician who runs the case) builds a positive reinforcement paradigm with the kid first, before any instruction starts. A positive reinforcement paradigm just means the kid wants to stay near you and the room you are in. A negative reinforcement paradigm means the kid is trying to escape you and that room. This work is the first phase before instruction. It is not a warm-up. It is not a five-minute pairing block at the start of session. It is a real phase with its own goals, its own data, and its own gating criteria. If you skip it, every program you run later has to fight gravity.
What Relationship-Based ABA Actually Means (and Why Pairing Is Not It)#
Pairing is the thing most of us were taught in our first week as a BT (behavior technician, the person running daily sessions). You sit on the floor with the kid, hand them snacks and toys, and try to make yourself fun. The idea is fine. The way it gets used is the problem.
So much of our field is obsessed with, you know, sometimes we call it pairing and pairing becomes almost transactional. I give you five minutes of fun. You give me X, Y, Z. And I knew that I wanted to go further than that. From the talk — Dr. Megan DeLeon
Relationship-based ABA is what you get when you stop treating pairing as a five-minute trade and start treating connection as the actual work. The kid does not owe you a target after the bubbles. The bubbles are not a coin you drop in a machine. You are building a person the kid trusts. Trust is not a transaction. It is a pattern of small moments where you showed up safe.
The clinical version of this thesis is simple. You are not in the room to get through programs. You are in the room to create a positive human experience for that kid, and then you teach inside that experience.
The Positive vs Negative Reinforcement Paradigm in One Plain Paragraph#
This is the technical anchor that keeps relationship-based ABA from sounding like vibes. The whole approach lives or dies on one paradigm contrast.
In a positive reinforcement paradigm, someone is connected to the environment and people are seeking to stay engaged and present. In a negative reinforcement paradigm, someone is trying to get away from the environment and people to get back to a better set of circumstances for themselves. From the talk — Dr. Megan DeLeon
Read that twice. A kid in a positive paradigm leans in. A kid in a negative paradigm leans out. Same room, same toys, same BT. The difference is whether the kid is choosing to be there. If the kid is trying to get away from you, no curriculum will save the session. The reinforcer you brought is being measured against the relief the kid would get from being somewhere else, and you will lose that fight every time. This is also the language you use in a clinical meeting when someone asks if relationship-based ABA is just being nice. It is not. It is a behavior-analytic choice about which paradigm the kid is operating under.
Why This Is Phase One, Not a Warm-Up#
The biggest mistake BCBAs make with this approach is treating it like a warm-up to real work. It is the work. It is also the gating criteria for the rest of the plan.
We are trained to get through a really long laundry list of different programs or IEP goals and things like that. And we lose sight of how important it is to put in the time and effort to build this really strong relationship first before we try to get to all of those other things. From the talk — Dr. Megan DeLeon
That laundry list is real. You stare at it on Sunday night. Twelve programs, four behavior goals, three IEP objectives the school is asking about. The pressure to start running it is high. The honest move is to put a phase line on your treatment plan that says: phase one is the relationship, phase two is everything else. Phase two does not start until phase one looks how it should look. That is not soft. That is the same logic you would use if you were waiting for a kid to mand reliably before starting tact training. You are waiting for a prerequisite skill set. The skill set just happens to live in you and the room, not in the kid.
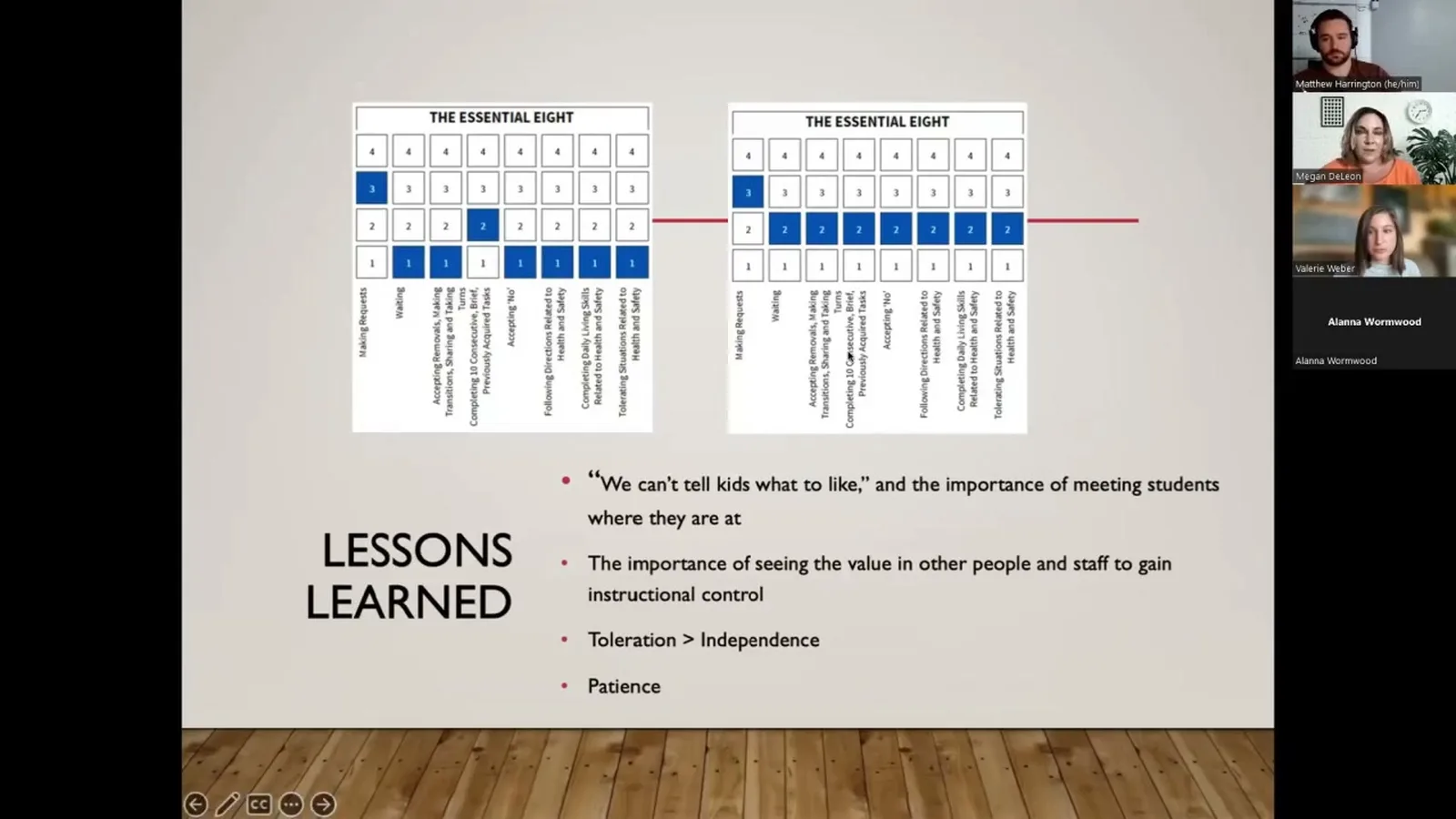
The Four Prerequisites You Have to See Before You Start Teaching#
The talk this page draws from frames four areas you need to see in place before instruction starts. They are: the kid is seeking you out, the kid is engaging with the environment, the kid stays present instead of escaping, and the kid will accept small bids for shared attention. These are observable. You can write them as data points. The kid approaches the BT within X seconds of session start. The kid sustains play for X minutes without trying to leave the room. The kid responds to a name call or a point. The kid will share a brief moment of joint attention on a toy you are holding.
If you do not see those four things, you do not yet have a teaching relationship. Adding more demands will not get you one. It will get you a negative reinforcement paradigm faster.
The practical version: run a free operant for the first stretch of every new case. Free operant just means the kid picks what they do and you follow. Track the four prerequisites as your data. When the data is stable, you have permission to start phase two. This is the same logic the NDBI (naturalistic developmental behavioral intervention, an umbrella that includes models like ESDM) literature uses. You earn the right to teach by first earning the kid's attention.
What Changes in Your Session Notes the Day You Switch Approaches#
The cleanest sign that you have actually moved to relationship-based ABA is that your session notes start to look different. Before the switch, your notes are a list of program names and percentages. After the switch, the first line of your note is about the kid's affect and approach. Did the kid run to the door? Did the kid stay in the play space? Did the kid offer you a toy? Those are not soft data points. They are the leading indicators of every percentage you will write below them.
This also changes how you talk in clinical meetings. Instead of saying the kid had a rough session, you say the kid was operating in a negative reinforcement paradigm for the first 20 minutes and we worked back to neutral by minute 35. That is a clinical sentence. It tells the team what to do next. It also tells the parents something they can feel, because they have seen the kid run from adults their whole life and they know what it looks like when it stops.
Where Relationship-Based ABA Fits With SBT, ESDM, and the NDBIs#
Relationship-based ABA is not a competing model. It is the layer underneath the model you are already using. SBT (skill-based treatment, the Hanley model) starts with a happy, relaxed, and engaged kid as its baseline. You cannot get there without phase one. ESDM (the Early Start Denver Model) is built on shared affect and joint activity routines. Same prerequisite. Every NDBI in the research base assumes the kid is leaning in, not running away. The relationship is the floor those models stand on.
So you do not have to pick. You build the relationship first, and then you run whatever model your team is trained in on top of it. The mistake is running the model without the floor. That is what produces sessions where the kid cries through DTT (discrete trial training, the structured teaching format) and the team blames the kid or the reinforcer.
What to Read Next If You Want to Defend This in Your Clinical Meeting#
If you walked into your next case review and your clinical director asked you to defend a slow start, here is what you need. You need the paradigm language from earlier on this page. You need the four prerequisites written as observable data points on your treatment plan. You need a phase line that says when phase two starts. And you need the closing thesis of the talk in plain language:
The things that Valerie and Alana have shared today and that you'll see in the additional case studies are the things we need to be focusing on, the human experience and creating that positive human experience for our clients and our students. From the talk — Dr. Megan DeLeon
That is the one-sentence version you can quote on Monday. Everything else on this site goes deeper into one piece of it. The rapport page covers what to do in the first ten sessions. The connection-based intervention page covers what session structure looks like when demands are off the table. The compassionate care page covers the assent piece. The client engagement page covers what to do when the reinforcer menu feels empty.
Frequently asked questions#
What is the difference between pairing and relationship-based ABA?
Pairing is a five-minute block at the start of session where you try to be fun. Relationship-based ABA is the whole phase before instruction starts. It can last days or weeks. It has its own goals, its own data, and its own gating criteria. The simplest test is this. If you would call your work done after one good play moment, you are doing pairing. If you would call it done only after the kid is consistently approaching, engaging, staying, and sharing attention, you are doing relationship-based ABA.
Is relationship-based ABA evidence-based?
The relationship piece is supported by research in behavior analysis, positive psychology, and developmental disabilities. The talk this page draws from cites Kelly and colleagues (2015) and LeBlanc and colleagues (2020) on pairing in ABA, plus work from the play therapy literature on building therapeutic alliance with autistic kids. The models that sit on top of it, like SBT and ESDM, have their own evidence bases. The cleanest answer for a clinical meeting is that relationship-based ABA is the prerequisite step the NDBI research base already assumes you have done.
How is this different from trauma-informed ABA?
There is heavy overlap. Trauma-informed ABA focuses on not adding to the kid's history of harm and on watching for signs the kid is dysregulated. Relationship-based ABA focuses on which reinforcement paradigm the kid is operating under and on the four prerequisites for teaching. In practice, a trauma-informed BCBA and a relationship-based BCBA make most of the same calls. They both run a free operant first. They both treat assent as a real signal. They both put phase one on the treatment plan before phase two.
Watch the full talk#
If this matches what you are seeing in your sessions, the full CEU walks through the process Dr. DeLeon and her colleagues developed, with case studies for kids of different ages and skill levels. It is free and counts for one general learning credit.
Watch the full CEU on relationship-based ABA